Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Eyeblink conditioning wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Central pattern generator wikipedia , lookup
End-plate potential wikipedia , lookup
Cortical cooling wikipedia , lookup
Aging brain wikipedia , lookup
Neuroplasticity wikipedia , lookup
Axon guidance wikipedia , lookup
Neuroeconomics wikipedia , lookup
Synaptogenesis wikipedia , lookup
Spike-and-wave wikipedia , lookup
Signal transduction wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Endocannabinoid system wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Synaptic gating wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Proprioception wikipedia , lookup
Cerebral cortex wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
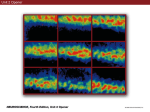
Neuro: 2:00 - 3:00 Monday, February 9, 2009 Dr. Weller Somatosensory Abbreviations: RF=Receptive Field; SA=Slowly Adapting; RA=Rapid Adapting I. Scribe: Taylor Nelson Proof: Chaz Capra Page 1 of 6 Key Points for Exam [S2] a. Key points for the exam, meaning multiple choice questions will come from these topics i. Somatosensory receptors ii. Dorsal column/medial lemniscal pathway iii. Traditional vs. current view of somatosensory areas iv. General functions for some of these areas of cortex v. Plasticity effects with deprivation,and the flip-side, increased use II. Relevant Concept: Stimulus Location [S3] a. One of the aspects of a stimulus in most of the sensory systems is knowing where it came from, location b. Receptors and the neurons they are connected with have a receptive field, a particular area in the periphery where application of a stimulus will cause the cell to respond c. Cell body of a neuron that goes out into the periphery where it gets input – in this case from the skin, which is the receptive field [S4] d. For the somatosensory system that would be the portion of the skin innervated or contacted by the receptor or accessory processes e. The density of the receptors (how many you have per square inch) and the size of their receptive field determines the special resolution or two-point touch discrimination i. Two-point touch discrimination is the ability to distinguish individual points of contact when touched simultaneously in two places ii. [S5] Areas of the skin that have the smallest two-point touch discrimination or the greatest acuity for detail in knowing where you’ve been touched have the greatest density of receptors (more receptors per square inch) – humans are most sensitive on the bottom surfaces of the hand and parts of the face, and least sensitive on back, calf, and thigh; meaning we have largest 2-point touch discrimination iii. The receptors in areas with the greatest acuity for detail must have smaller receptive fields to fit them all in III. Title [S6] a. These receptive fields form topographic maps b. For touch, theses maps are called somatotopic (somato meaning body) maps i. Formed by orderly arrangement of receptive fields as they project into central parts of the somatosensory system c. These maps often have what are called congruent borders d. They are not an exact replication of the skin surface because parts of the skin surface that we use to make fine tactile discriminations are magnified or enlarged in the maps e. [S7] These are two of the areas of the somatosensory cortex of an owl monkey i. Owl monkeys are nice because they practically have no sulci, so it is easier to see things right on the surface ii. Two maps, areas 3b and 1 of the somatosensory cortex iii. Roughly the skin of the opposite side of the body is represented from foot, leg, trunk, arm, hand, and face iv. A congruent border is here, that means these maps often reverse at a common border 1. Reverse at the congruent border (congruent means shared) 2. The maps have a large area devoted to the hands and a large area for input from the face 3. Maps typically have a reversal, so when mapping the cortex you know you are going into another area f. [S8] Cartoon showing what animals would look like if the area devoted to cortex matched what was on the skin surface – illustrates the concept of magnification i. In the rabbit somatosensory areas the skin of the face is magnified or enlarged ii. Cat – face, paws iii. Monkey – face, hands iv. Humans – hands, face, and especially intraoral surfaces and we think this relates to language IV. 4 Perceptual Modalities [S10] a. The somatosensory system actually encompasses four perceptual modalities, only two will be discussed i. Tactile or cutaneous sense – how we commonly use the word touch, this is the sense by which you can identify things when you run your hand over them, for discriminative touch – distinguishing size, shape, and texture of an object ii. Proprioception – refers to deeper receptors, these are receptors that are in joints and muscles and allow you to know what your body position is when your eyes are closed and you are not moving (static) and when you are moving, this information is very important in movement and maintaining posture; also used with touch Neuro: 2:00 - 3:00 Monday, February 9, 2009 Dr. Weller iii. Will not discuss thermal or pain Somatosensory Scribe: Taylor Nelson Proof: Chaz Capra Page 2 of 6 V. Somatosensory Receptors [S11] a. Mechanoreceptors b. Receptors/receptor complex generate action potentials as well as doing the transduction c. There is a key distinction between rapidly and slowly adapting kinds of receptors i. These will be located in different parts of the skin and have different sizes of receptive fields VI. Principal Types of Tactile or Cutaneous Receptors [S12] a. Most are Encapsulated – covered with some peripheral tissue, typically some kind of epithelial tissue to form a complex i. Meissner corpuscle ii. Pacinian corpuscle iii. Ruffini ending b. Nonencapsulated i. Merkel ending VII. Mechanoreceptor distribution in hairy and glabrous skin [S13] a. Hairy skin on the left (will not discuss), smooth or glabrous skin on the right b. Some of these receptors are superficial in the skin and others are deeper in the skin i. The two of the four receptors that are superficial in the skin are the Meissner corpuscle and the Merkel disc/receptor ii. The two that are deeper in the skin are the Pacinian corpuscle and the Ruffini ending c. Of the four kinds of receptors superficial in the skin you will have one rapidly adapting and one slowly adapting and deeper in the skin you will also have one rapidly adapting and one slowly adapting so everything is covered in both locations VIII. 2 Rapidly Adapting Touch Receptors [S14] a. The rapidly adapting receptors respond to the onset of the touch and also usually the offset b. Superficial Meissner corpuscle i. Small RFs, 40% in hand, for touch, edges, flutter, texture as coarser objects moved across skin, adjustment of grip c. Deeper Pacinian corpuscle i. Bigger RFs, 10-15% in hand, for vibration, movement of fine-textured objects across skin IX. 2 Slowly Adapting Touch Receptors [S15] a. Slowly adapting receptors are not just active when you touch something but also when you continue to have contact with it b. Superficial Merkel ending/epithelial cell complex i. Small RFs, 25% in hand, for touch, static edges, shapes, rough texture c. Deeper Ruffini ending i. Bigger RFs, 20% in hand, for shape of grasped object, pressure X. 4 Cutaneous Receptors [S16] a. Nice slide that summarizes some of the features of the different kinds of receptors i. Superficially in the skin we have Meissner’s corpuscle and Merkel cells, deep in the skin we have Pacinian corpuscle and Ruffini endings ii. Note the sizes of their receptive fields 1. It should come as no surprise that the receptors closer to the surface have smaller receptive fields 2. Receptors deeper in the skin have larger receptive fields, more diffuse 3. Of the superficial receptors in the skin one is rapidly adapting and one is slowly adapting, the bar represents when the different receptors would fire during a constant stimulus – as stated earlier the rapidly adapting will fire at the onset and offset of the stimulus and the slowly adapting will continue to fire through the duration of contact, the same is true of the receptors deep in the skin b. Summary [S17] i. Superficial skin has Merkel endings (SA) and Meissner corpuscles (RA), both with small RFs; for detailed stimuli like Braille dots ii. Deeper skin has Ruffini endings (SA) and Pacinian corpuscles (RA); note: not “deep” as proprioceptors which lie in the joints and muscles, all of these receptors are cutaneous so deep here refers to deep in the skin XI. Proprioception [S18] a. Detects stationary body position and movement (kinesthesia); for evaluating shape of objects, controlling movements b. Just two main types of proprioceptors: Neuro: 2:00 - 3:00 Scribe: Taylor Nelson Monday, February 9, 2009 Proof: Chaz Capra Dr. Weller Somatosensory Page 3 of 6 i. Muscle spindles – in muscles ii. Golgi tendon organs – ends of the muscles in tendons c. Can tell where they are by their names XII. Muscle Spindles [S19] a. Long, thin stretch receptors in striated (voluntary) muscle b. Consist of few small intrafusal (meaning within the muscle) muscle fibers covered by central capsule c. Ends of intrafusal muscle fibers attached to extrafusal muscle fibers (so connected in parallel) d. Detect stretch or lengthening of muscle which lengthens the intrafusal fibers; if the muscle is extended, these would be excited and fire e. [S20] Intrafusal muscle fibers are located within the body of the muscle fibers and they contain the muscle spindles i. Receptor is connected in parallel with the other muscle fibers and it detects stretch ii. [S21] Knee jerk reflex is due to activation of the muscle spindles 1. When the knee is taped with the hammer that stretches/lengthens the quadriceps which activates the muscle spindle and you have a simple reflex in the spinal cord that causes contraction of the quadriceps muscle, it shortens and that’s why you kick your leg out XIII. Golgi Tendon Organs [S22] a. Golgi tendon organs are found at the ends of the muscles so they are connected in series with the muscle b. Sensory fibers kind of branch and become entwined with collagen tissue in the tendon c. They detect muscle contraction i. When the muscle is used or shortened that’s when the Golgi tendon organs are activated ii. Opposite of muscle spindles XIV. Relation of Modalities to Afferent Fiber Size [S24] a. How do these receptors send information on into the nervous system b. Different kinds of nerves carry different information i. Discovered by Henry Head, 1920’s ii. He cut his own peripheral nerves and noted that there was a difference in the time course of recovery of cutaneous versus pain and temperature iii. This suggested that this kind of information was carried by different nerves c. Erlanger and Gasser, 1927, used a oscilloscope to show the conduction velocity or the speed of action potentials and found that cutaneous touch was carried by thicker myelinated axons and transmitted faster compared to pain and temperature which is carried by thinner and commonly unmyelinated axons d. Nomenclature – fastest to slowest: A to C or I to IV XV. Generalities [S26] a. Only talking about the somatosensory pathway for touch and proprioception (pain and temperature will come later) b. For all pathways should know where the first, second, and third neurons are i. Know where the cell bodies are, where the synapses occur, where crossing occurs, etc. c. For this pathway the primary neuron’s cell body is in the dorsal root ganglia for spinal nerves or for input from the head (cranial structures) in the trigeminal ganglion d. The cell body is a pseudounipolar neuron that branches and has one part going out to the periphery and the other acts as the real axon sending information centrally into the spinal cord e. Input for the neurons comes from regions of the skin called dermatomes [S27] i. A spinal nerve would get input from a strip of skin ii. Dermatomes running down the arms and legs are mainly longitudinal whereas the dermatomes of the trunk are horizontal iii. If you ever have had a pain or sciatica, the pain would follow these dermatomes XVI. Fine touch or dorsal column/medial lemniscal pathway [S28] a. Named such because it travels up the dorsal column of the spinal cord and once it crosses over at the level of the brainstem it travels up the medial lemniscus b. Axons from primary neurons enter spinal cord via dorsal roots and ascend ipsilaterally in dorsal columns which are also called medial gracile (lower body) and lateral cuneate (upper body) fasciculi c. Synapse on 2nd order neurons at the level of the lower medulla in gracilis and cuneatus nuclei, the cuneate fasiculi go to the cuneatus nucleus and the gracile fasiculi go to the gracilis nucleus d. Axons of 2nd order neurons cross and ascend in medial lemniscus to synapse on 3 rd order neurons in Ventroposteriorlateralis (VPL) nucleus of thalamus e. Axons of 3rd order neurons ascend via internal capsule to somatosensory cortex in parietal lobe i. Above pictured in [S29] Neuro: 2:00 - 3:00 Scribe: Taylor Nelson Monday, February 9, 2009 Proof: Chaz Capra Dr. Weller Somatosensory Page 4 of 6 XVII. Details [S31] a. What about input from the skin of the head and the face (input from the trigeminal nerve)? b. Trigeminal input goes to principal trigeminal nucleus in the pons instead of the gracile and cuneate nuclei c. 2nd order neurons’ axons cross and ascend in medial lemniscus to 3rd order neurons in ventroposteriormedialis (VPM) of thalamus (saw the VPM of thalamus in taste lecture) d. VPM neurons project to somatosensory cortex in the parietal lobe e. All structures have somatotopic maps with magnification of particular body parts where you have more receptors XVIII. Thalamus: Ventroposterior Complex [S33] a. When we call it the ventroposterior complex, we use complex because it has two parts i. Lateral part which gets input from skin on the opposite side of the body ii. Medial part that gets input from skin on the opposite side of the head b. [S34] Named ventroposterior because its ventral and a little posterior i. Lateral part is VPL ii. Medial part is just medial to VPL XIX. Cartoon [S35] a. “Mammunculus” b. How the skin of the mammal would be represented in VPL and VPM of thalamus i. Head is represented in VPM medially, it’s magnified XX. How areas of cortex defined: multiple criteria [S37] a. If an area of cortex does something unique it will have a distinctive architecture i. [S39] Lateral view of a monkey brain 1. If we took a section of tissue from primary visual cortex and stained it with crystal violet you would see something like this – the cortex forms horizontal layers, you will have denser accumulations of cells and the cells may differ in size of cell bodies. 2. This histological appearance is called cytoarchitecture because it’s looking at cell body location 3. Brodmann used this to come up with his map of the cortex [S40] a. He identified about 52 areas for the human cortex b. Somatosensory areas are areas 3,1,2,5,and 7 c. Brodmann used horizontal sections through the cortex to identify different areas, so in general the areas at the top have low numbers and the areas on the bottom have high numbers b. Will have a certain map or representation of the periphery c. Will have a unique set of neural properties d. Will have a unique pattern of connections with other areas of cortex and subcortical structures e. All of this will culminate by making a unique contribution to function XXI. Traditional View of Sensory Cortex [S38] – Contrast traditional and Current views of somatosensory cortex = EXAM QUESTION a. Woolsey and collaborators (1937, 1941) used evoked potentials or macroelectrode recording of large regions of cortex b. Found single “S1” map encompassing 4 of Brodmann’s (1909) cytoarchitectonic areas: 3a, 3b, 1, and 2 (puzzling) – came to this erroneous conclusion due to crude methods that did not allow them to see a lot of detail c. We believe there are at least 200 different areas of cortex that do different things so this result is going in the wrong direction as Woolsey said that there is one map that covers four of Brodmann’s areas d. This map formed basic somatotopic organization, used the term “-unculus”, with medial (tail) to lateral (head) organization e. Differential magnification in different areas for different species f. [S42] Adrian (1941) reported ventral “S2”, in parietal operculum or insula (bottom of Sylvian or lateral fissure) g. Woolsey did somatosensory mapping in a range of mammals and concluded they all had only S1 and S2 i. This is the traditional view, that all animals have just two areas of somatosensory cortex h. Penfield and collaborators (1950, 1954) “confirmed” SI homunculus in humans using electrodes on epilepsy patients i. Reported genitals represented on the medial wall by the feet XXII. Current View [S44] a. Arose when people used delicate microelectrodes and picked the right animal to study (smooth-brained owl monkey) b. Not just 2 somatosensory areas of cortex, but 5 in lower mammals, > 8-10 in primates, including humans c. Woolsey’s “SI” not 1 but 4 areas in primates, corresponding to Brodmann’s areas 3a, 3b, 1, and 2 (puzzle resolved) – Brodmann was right! Neuro: 2:00 - 3:00 Scribe: Taylor Nelson Monday, February 9, 2009 Proof: Chaz Capra Dr. Weller Somatosensory Page 5 of 6 d. Not just 1 area, “SII”, in parietal operculum, but at least 2 areas (SII, Parietal Ventral or PV) e. Also areas behind area 2: areas 5 and 7 f. [S45] Photo/diagram of areas described above g. Many areas in humans because of specialization of function, presumably the different areas make different contributions to somatosensation XXIII. Details about “SI” [S46] a. Areas 3b and 1 have clearest maps because they get mainly light touch cutaneous input b. 3b and 1 maps share a congruent border and are roughly mirror reversals c. Differential magnification of important body parts, with species differences i. Whiskers of rats vs. squirrels; paws of raccoons vs. cats; rays of star-nosed mole; incisors of naked mole rat; ventral hand, face, tongue of humans d. Correctly identified the location of the genitals, not medial to the feet but in order where they belong XXIV. Somatosensory specializations result in magnification in maps [S48] a. Various examples of magnification resulting from an expanded map b. [S49] Mouse or Rat unculus with a 1:1 correspondence of each whisker and its representation in the brain XXV. [S50] a. Areas 3b and 1 i. Cutaneous input (minor pain and temperature) ii. With removal of 3b and 1 in monkeys, deficits in fine touch b. Areas 2 and 3a i. Proprioceptive input from muscle spindle and Golgi tendon (also some cutaneous input from cortex) ii. Should know where these are located, 3a in front of 3b and area 2 is behind area 1, so straddling the cutaneous areas c. Damage to 3a, 3b, 1, and 2: deficits in tactile discrimination and proprioception XXVI. [S52] a. SII and PV are involved in more complex somatosensory abilities involving tactile touch learning, transfer between the hands, etc. XXVII. Cortical Areas Consist of Columns [S53] a. All of the neurons in a column would do the same thing, they would get inputs from the same receptive field b. Discovered first in the somatosensory system in the 1950s c. Columns exists because neurons in a vertical penetration mainly make connections up and down XXVIII. Details about Connections [S55] a. Serial and parallel processing b. 1 cortical area receives input from multiple thalamic sources, 1 thalamic nucleus projects to several cortical targets XXIX. Plasticity in the Somatosensory System [S57] a. Traditional dogma: plasticity only occurs in young brains, old brains are rigid and cannot adjust to injury i. Came from studies done in rats – if a row of vibrissae or whiskers in a newborn rat areas of cortex that got input from that removed row would be totally taken over by input from adjacent vibrissae; this was not found if you did the same in an adult rat b. [S61] New view: plasticity also in mature brains i. If a nerve is cut in an owl monkey you will see little differences right away but if you waited some months you would see the map was reorganized and some of the other areas would have taken over the input to the lost nerve 1. [S63] Two stages in the changes seen a. Small changes right after the nerve cut b. Greater changes long term i. 2 implied different mechanisms 1. Immediate: unmasking of latent inputs, disinhibition 2. Delayed: sprouting, growth of connections, synaptic modifications ii. [S64] Also found variability in hand maps in different normal owl monkeys: implies each brain unique iii. Increased usage induces changes in maps 1. Repetitive finger stimulation, nursing rats[S65] iv. [S66-67]Silver springs monkeys – big scale change, nerves cut to entire hand thus the expansion was too great for the cortex to cover so found changes all along the way v. [S69] Findings in Humans 1. People who have lost an arm have reported that when the skin of their face is touched it feels like the missing arm is being touched a. The cortical face area has taken over the input that should have gone to missing arm Neuro: 2:00 - 3:00 Scribe: Taylor Nelson Monday, February 9, 2009 Proof: Chaz Capra Dr. Weller Somatosensory Page 6 of 6 2. Changes due to surgery for syndactyly a. Compressed representations of fingers expanded 3. Changes due to increased use a. Functionally: Ebert, Taub et al. (1995), increased cortical representation of fingers D2-5 in left hand of stringed instrument players b. Structurally: Gauthier et al. (2008), increased cortical area devoted to stroke-affected arm after constraint-induced (CI) therapy [END 54:18]