Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Schizophrenia wikipedia , lookup
Addictive personality wikipedia , lookup
Rumination syndrome wikipedia , lookup
Broken windows theory wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Obsessive–compulsive disorder wikipedia , lookup
Memory disorder wikipedia , lookup
Psychological trauma wikipedia , lookup
Impulsivity wikipedia , lookup
Behavioral theories of depression wikipedia , lookup
Obsessive–compulsive personality disorder wikipedia , lookup
Eating disorders and memory wikipedia , lookup
Biology of depression wikipedia , lookup
Autism spectrum wikipedia , lookup
Anxiety disorder wikipedia , lookup
Social anxiety disorder wikipedia , lookup
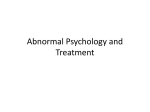
Panic disorder wikipedia , lookup
Major depressive disorder wikipedia , lookup
Eating disorder wikipedia , lookup
Personality disorder wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
Depersonalization disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Bipolar II disorder wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Bipolar disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
Munchausen by Internet wikipedia , lookup
Schizoaffective disorder wikipedia , lookup
Diagnosis of Asperger syndrome wikipedia , lookup
Conduct disorder wikipedia , lookup
Antisocial personality disorder wikipedia , lookup
Mental disorder wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Spectrum disorder wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
Child psychopathology wikipedia , lookup
Treatment of bipolar disorder wikipedia , lookup
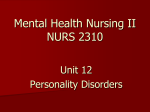
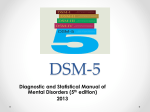
Myers’ PSYCHOLOGY (7th Ed) Chapter 16 Psychological Disorders James A. McCubbin, PhD Clemson University Worth Publishers 1 http://www.appsychology.net/flash/index.shtml Good AP Psy website for review! ------------------------------------------------------------------------ Ch. 16: Psy Disorders: “harmful dysfunction” in which behavior is judged to be… A. Atypical (violates social-norms): goes against accepted behaviors; but not enough by itself to be a mental disorder… ---Varies w/ era & culture B. Disturbing: causes distress to you or those around you-C. Maladaptive—harmful; keeps you from functioning well in your world D. Unjustifiable: no apparent reason….sometimes there’s a good reason 2 Defining Psychological Disorders Psychological disorders Deviant behavior Distressful behavior Harmful dysfunctional behavior Definition varies by context/culture Attention deficit hyperactivity disorder (ADHD) Historical Perspective Formerly Perceived Causes movements of sun or moon lunacy--full moon evil spirits; demons ; witches Ancient Treatments exorcism, caged like animals, beaten, burned, castrated, mutilated, blood replaced w/ animal’s blood Lock into attics…chain them up Changing from “demons” to illness: -Paris: Philippe Pinel: became head of a mental hospital in 1700’s & saw horrid ways patients were treated…unchained the people & demanded humane treatment BEGAN the MEDICAL MODEL 4 Psychological Disorders Medical Model concept that diseases have physical causes can be diagnosed, treated, (& in most cases) cured assumes “mental” illnesses can be diagnosed on the basis of their symptoms & cured through therapy…& may include treatment in a psychiatric hospital Used to use psych. hospitals a lot but now most is on out-patient basis Bio-Psycho-Social Perspective: assumes that biological, socio-cultural, & psychological factors combine & interact to produce psychological disorders --a combination of causes in a cycle 5 Psychological Disorders 6 Psychological Disorders--Etiology Etiology: the causes of a disorder or condition (where it comes from…) DSM-IV: classifies a disorder…mainly the symptoms that define that disorder American Psychiatric Association’s Diagnostic & Statistical Manual of Mental Disorders (4th Edition) = DSM-IV-TR (text revision...this is latest) a widely used system for classifying & defining what constitutes a particular psychological disorders It does NOT tell you how to treat a disorder 7 Classifying Psychological Disorders Labeling Psychological Disorders Rosenhan’s study Power of labels Preconception can stigmatize Insanity label Stereotypes of the mentally ill Self-fulfilling prophecy Match the Famous ppl w/ mental disorder http://health.discovery.com/tv/psych-week/articles/celebrities-mentaldisorders.html NOTE: Some may have more than 1 disorder, some disorders have more than one person affected ADHD Agoraphobia Bipolar Disorder Bulimia Depression DID (Dissociative identity disorder) OCD (obsessive compulsive disorder) Panic Attacks Post-partum depression Schizophrenia Social Anxiety Substance Abuse (answers on LAST slide) Joan Baez Craig Ferguson Paula Deen Howard Hughes Brooke Shields Vincent van Gogh Emma Thompson Michael Phelps Elton John Herschel Walker Carrie Fisher John Nash 11 Psychological Disorders- Etiology When Revisions are made in the DSM : EX: used to classify homosexuality as a mental disorder but when they did the last major revisions (late ’70’s) it was changed & is no longer considered a disorder Neurotic Disorder: usually distressing/upsetting but… allows one to think rationally & function socially (this term is seldom used now) Psychotic disorder Person loses contact w/ reality, experiencing irrational ideas & distorted perceptions Commonly seen in schizophrenia & more severe bipolar disorders as well as others Major divisions of mental disorders (there are others): *anxiety disord. *schizophrenia *dissociative disord. *mood disorders *personality disord. *somatoform 12 More clarification of psychosis vs. neurosis: Psychosis: A loss of contact with reality, usually including delusions & hallucinations. Can be caused by drugs (using & withdrawal), brain tumors, dementia & other brain diseases..plus certain psychiatric disorders Neurosis: a relatively mild mental illness that is not caused by physical disease, involving symptoms of stress (EX: depression, anxiety, obsessive behavior, hypochondria) but not a radical loss of touch with reality. This term was taken out of DSM in 1980 & is not used much today in true diagnoses…used more as a descriptive term if at all. 13 Anxiety Disorders: distressing, persistent anxiety or maladaptive behaviors that reduce anxiety for no apparent or rational reason (these are not rare…) Panic Disorder (panic attacks): marked by a minuteslong episode of intense dread in which a person experiences terror and accompanying chest pain, choking, or other frightening sensation Often diagnosed in ER…why? Generalized Anxiety Disorder: person is tense, apprehensive, and in a state of autonomic nervous system arousal Phobia: persistent, irrational fear of a specific object or situation Agoraphobia: fear of unfamiliar places…fear of being away from home Obsessive-Compulsive Disorder: unwanted repetitive thoughts (obsessions) and/or actions (compulsions)14 Obsessive-Compulsive Disorder Obsessive-compulsive disorder An obsession versus a compulsion Checkers Hand washers PTSD: Post Traumatic 16 Anxiety Disorders: NOTE: There are many more than just those most common ones on the previous slide… Common & uncommon fears: extremes = phobias 17 Anxiety Disorders: OCD obsessions & compulsions: Kids & adolescents 18 Explaining anxiety disorders: etiology– cause? fear conditioning: bad uncontrollable events can cause these (rape victim?) EX: PTSD: post-traumatic stress disorder stimulus generalization: person falls…then fears airplanes… reinforcement: becomes cyclic: anxiety, so do something to relieve it (run away, stay home, etc.), feel better, so you will do this the next time observational learning: parents, siblings, etc. teach fears to the young genetic: thru natural selection (many are heritable) physiological: folks w/ overactive limbic system can be prone to these disorders…& antidepressants help them 19 Anxiety Disorders PET Scan of brain of obsessive/ compulsive disorder (OCD) High metabolic activity (red) in frontal lobe areas involved with directing attention Over-active amygdala &/or limbic system can affect this ** b/c it’s a stimulant, nicotine increases risk of a 1st episode of anxiety disorders 20 Mood Disorders: Emotional extremes (ups OR downs) Mild or moderate Depression (aka dysthymic disor.): “common cold” of mental disorders… Related to lack of N-T’s serotonin & nor-epinephrine (both affect mood) Women more prone to depression…probably b/c of ... **Hormones **Lack of self-esteem **Lack of a a sense of efficacy ( “I have control, etc.) Major Depressive Disorder For no apparent reason, person experiences 2 or more wks of depressed moods, feelings of worthlessness, & diminished interest or pleasure in most activities Possibility of suicide is major concern If drugs & cognitive/behavioral therapy don’t work, this is 1 of few disorders Dr’s. may still use shock (ECTelectroconvulsive) therapy on b/c of fear of suicide 21 Mood Disorders Manic Episodes (“Mania”) Marked by a hyperactive, wildly optimistic state Biological influence seems to be excess of what 2 neurotransmitters? ( ___ & especially ___ ) EX’s of manic behaviors: Could be 1, some, or all (or some other…) of the following: -grandiose ideas -euphoric optimism -spending sprees -reckless, aggressive -long periods of no sleep -speech becomes loud -excessive self-esteem -poor judgment, egocentric -increased chances of unprotected sex 22 Bipolar Disorder Mood disorder in which the person alternates betwn. the hopelessness & lethargy of depression… & the overexcited state of mania way up…then way down…& back again… formerly called manic-depressive disorder 23 Bipolar disorder: a lifelong illness. Episodes of mania and depression eventually can occur again, if you don't get treatment. Many continue to have symptoms, even after getting treatment Types of bipolar disorder: Bipolar I disorder: involves periods of severe mood episodes from mania to depression. Bipolar II disorder: a milder form of mood elevation, involving milder episodes of hypomania that alternate with periods of severe depression. Cyclothymic disorder: periods of hypomania with brief periods of depression that are not as extensive or long-lasting as seen in full depressive episodes. Mixed bipolar: periods that simultaneously involve the full symptoms of both a manic and a full depressive episode. It's marked by grandiose feelings with racing thoughts. At the same time, the person is irritable, angry, moody, and feeling bad. 24 Rapid-cycling bipolar disorder: Characterized by 4 or more mood episodes that occur within a 12month period. Episodes must last for some minimum number of days in order to be considered distinct episodes. MAY experience changes in polarity (high low or vice-versa) within a single week, or even within a single day -- the full symptom profile that defines distinct, separate episodes may not be present (EX: the person may not have a decreased need for sleep), making such "ultra-rapid" cycling a more controversial phenomenon. Rapid cycling can occur at any time in the course of illness, although some researchers believe that it may be more common at later points in the lifetime duration of illness. Women appear more likely than men to have rapid cycling. A rapidcycling pattern increases risk for severe depression and suicide attempts. Antidepressants are thought to trigger and prolong rapid cycling in bipolar disorder. However, that theory is controversial and is still being studied. 25 Mood Disorders-Bipolar PET scans show that brain energy consumption rises and falls with emotional switches May 17 Depressed state May 18 Manic state May27 26 Depressed state Manic Chocolate deliveries.. 27 READ!! P.638 Suicides & differing groups: National: see #’s: where’s US? Racial: Euro.-Amer.(W) more than Afr. Amer. (B) Gender: Which try? Which succeed? Why? Age: most = older men; increase in older male teens Other groups: religious vs. non-relig. heterosexual/homosexual? married, single, widowed, divorced? drug usage? The Depressed brain: How do serotonin & norepinephrine affect depression vs. mania?? 28 Mood Disorders - Depression & Gender cross-culturally: Females more susceptible 29 Mood Disorders-Depression Canadian depression rates: M vs F in varying ages 30 Mood DisordersSuicide 31 Mood Disorders-Depression Altering any one component of the chemistry-cognitionmood circuit can alter the others Genetic: there is a strong genetic link in mood disorders Physiological (638) brains differences: lobes, NT’s, activity levels Social-cognitive: selfdefeating beliefs; negative thoughts -”stable, global, internal” (b-640) 32 Mood DisordersDepression The vicious cycle of depression can be broken at any point Rumination: dwelling on something P. 643: Loneliness: “aloneness often breeds loneliness”: -excluded -unloved -constricted -alienated 33 Major Depressive Disorder Bipolar Disorder Bipolar Disorder Mania (manic) Overtalkative, overactive, elated, little need for sleep, etc. Bipolar disorder and creativity 2 other Mood disorders: Post-Partum Depression: “baby blues”…comes after birth of a baby…linked to hormonal changes (Brooks Shield, Andrea Yates) SAD: seasonal Affective Disorder: “Winter Blues”—lack of light usually the trigger -hormone melatonin linked to this it also helps w/ jetlag, shift work— i.e., disruption of sleep cycles 36 Understanding Mood Disorders Many behavioral and cognitive changes accompany depression Depression is widespread Compared with men, women are nearly twice as vulnerable to major depression Most major depressive episodes self-terminate Stressful events related to work, marriage and close relationships often precede depression With each new generation, depression is striking earlier and affecting more people Understanding Mood Disorders The Biological Perspective Genetic Influences Mood disorders run in families Heritability Linkage analysis The depressed brain Biochemical influences Norepinephrine and serotonin Understanding Mood Disorders The Social-Cognitive Perspective Negative Thoughts & Moods Interact Self-defeating beliefs Learned helplessness Overthinking Explanatory style Stable, global, internal explanations Cause versus indictor of depression? Understanding Mood Disorders: Explanatory Styles Understanding Mood Disorders The Social-Cognitive Perspective Depression’s Vicious Cycle Stressful experience Negative explanatory style Depressed mood Cognitive and behavioral changes Understanding Mood Disorders The Vicious Cycle of Depression Biopsychosocial Approach to Depression Dissociative Disorders (Read 644-5) conscious awareness becomes separated (dissociated) from previous memories, thoughts, and feelings Dissociative amnesia: blocking of information regarding a very stressful event; just go on w/ life like it never happened (Freud’s repression) Dissociative Fugue: go to new place & take up new life after some traumatic event Dissociative Identity Disorder (DID) rare dissociative disorder in which a person exhibits two or more distinct and alternating personalities formerly called multiple personality disorder Some psychologists disbelieve this, say it’s role-playing It is NOT schizophrenia (though you’ll hear it called that) V. rare & disputed by most psychologists Virtually always related to long-term childhood sexual abuse 44 Dissociative Identity Disorder Dissociative identity disorder (DID) Multiple personality disorder Understanding Dissociative Identity Disorder Genuine disorder or not? DID rates…v. small: .01% Therapist’s creation? Ppl do not come “with” the disorder—often comes after therapist begins to ask specifically about it Differences from culture to culture are too great…it is NOT cross-cultural & seems specific mainly to USA DID and other disorders Schizophrenia Schizophrenia: This one IS real…& v. sad… literal translation “split mind” which is why may hear schiz. called multi. personality a group of severe disorders characterized by: disorganized and delusional thinking disturbed perceptions inappropriate emotions and actions Delusions false beliefs, often of persecution or grandeur, that may accompany psychotic disorders Hallucinations sensory experiences without sensory stimulation47 Schizophrenic Art: also 48 49 5 subtypes of schizophrenia: Also… Acute vs. chronic? 50 Schizophrenia 51 Schizophrenia in ID Twins: 1 w/ & 1 w/o Indicates some other cause other than ____? FLUID FILLED areas are “ventricles”…larger ventricles associated w/ schizophrenia 52 Positive vs. negative symptoms … These do NOT relate to good or bad… Positive: something added… EX: hallucinations; delusions; excessive emotion….etc. Negative: something taken away… EX: -flat affect (no emotion) -no movement (catatonic) Onset of schiz.: those predisposed to schiz. have their 1st episode typically between about ages 17 – 35 --some possible warning signs… EX: poor selective attention 53 Understanding Schizophrenia: Psychological Factors Possible warning signs Mother severely schizophrenic Birth complications (low weight/oxygen deprivation) Separation from parents Short attention span Poor muscle coordination Disruptive or withdrawn behavior Emotional unpredictability Poor peer relations and solo play Clarification: Positive vs. Negative Schiz. symptoms Positive symptoms are things that are present in schizophrenics which are absent in normal people, such as delusions, hallucinations, or word salad. Negative symptoms are things which are absent in schizophrenics which are present in normal people, such as flat affect, avolition (lack of motivation, etc.) or catatonia. 55 Etiology of schizophrenia: Environment: Other disorders have effects from from the environment, BUT schiz. very much physiological …BUT stress can bring on episodes in those who have physiological tendencies already EX: family interaction & communication can have an effect (Hi-risk factors RE: schiz.: p. 652) Dopamine over-activity: too much dopamine in brains of schiz. during autopsies Brain anatomy: low activity in frontal lobes; enlarged brain cavities (ventricles) Maternal viruses during mid-pregnancy: is it the virus, or the medications, etc.? But only 2% of schiz. seem affected this way… Genetic factors: there is a genetic link …so if you have a close family member w/ schiz., risk is up 56 Personality Disorders: inflexible, long-lasting behavior patterns that impair social functioning usually without anxiety, depression, or delusions (SOME below......BUT are others!) Borderline Personality Disorder: manipulative; can be sexually promiscuous; defensive; high-risk; may threaten suicide for attention Co-dependent Persn. Disor.: over-dependent on another; will allow another to abuse verbally, emotionally, etc., & tend to make excuses for him/her -usually women; “passive-aggressive” Narcissistic Persn. Disor.: It’s ALL about MEEEE!!! Antisocial Persn. Disor. (aka “sociopaths”) person (usually male) exhibits a lack of conscience for wrongdoing, even toward friends & family may be aggressive and ruthless or a clever con artist 57 Early signs? (See “ppl who abuse animals…”) A personality disorder : Enduring pattern of inner experience & behavior that deviates markedly from the expectations of the individual’s culture, is pervasive & inflexible, has an onset in adolescence or early adulthood, is stable over time, and leads to distress or impairment. From DSM-5 Dimensional Models for Personality Disorders General Personality Disorder Paranoid Personality Disorder Schizoid Personality Disorder Schizotypal Personality Disorder Antisocial Personality Disorder Borderline Personality Disorder Histrionic Personality Disorder Narcissistic Personality Disorder Avoidant Personality Disorder Dependent Personality Disorder Obsessive-Compulsive Personality Disorder Other Specified Personality Disorder Unspecified Personality Disorder Personality Change Due to Another Medical Condition 58 Anti-social personality disorder: little guilt or effect Boys who were later convicted of a crime showed relatively low arousal during stress situations 59 Antisocial-Personality Disorders PET scans illustrate reduced activation in a murderer’s frontal cortex…lacks guilt, etc. Less related to genetics, more environ. Normal Murderer 60 Personality Disorders: Do seem to have an environmental etiology...often abusive, poor, neglectful parents are involved + birth problems 61 Rates of Psychological Disorders: Highest? Lowest? Cultural /gender aspects? 62 Rates of Disorders Mental health statistics Influence of poverty Other factors Somatoform disorders: (Not in bk!) -Preoccupation w/ health…or showing physical symptoms w/ NO true physical problems Conversion disorder: used to be called “hysterical ___”, i.e., hysterical blindness or hysterical paralysis Hypochodriasis: hypochondria…preoccupied w/ your health, worried you have everything Munchausen’s Syndrome or Munchausen by proxy: actually poison or otherwise hurt yourself (or another= proxy) in order to get sympathetic attention (any movie you remember?) 64 65 Answers to Match the famous ppl w/ mental disorders ADHD: Michael Phelps Agoraphobia: Paula Deen Bipolar Disorder: Carrie Fisher, Vincent van Gogh Bulimia: Elton John Depression: Emma Thompson Dissociative identity disorder (DID): Herschel Walker OCD: Howard Hughes Panic Attacks: Paula Deen Post-partum depression: Brooke Shields Schizophrenia: John Nash Social Anxiety: Joan Baez Substance Abuse: Craig Ferguson, Elton John 66