Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
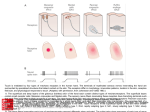
Lecture 7 Somatosensory System stimulus receptors neural pathways plasticity perception "Body senses" Cutaneous: detection of stimuli on skin Kinesthetic: detection of internal conditions: body position & movement receptors in joints, tendons & muscles Cutaneous: Stimulus: pressure on skin temperature mechanoreceptors -- sensitive to physical distortion Sensitivity: skin is sensitive to bumps that are only .006 mm high, .04mm wide (that’s 6 X 40 microns!) Types: (16.2) Pressure/Light touch/vibration Pacinian corpuscle -deep in dermis of skin large: can be 2mm long X 1 mm in diameter onion-like large receptive fields - entire finger or 1/2 of palm rapidly adapting vibration - 200-300 Hz = best frequency Ruffini endings small Pacinians large receptive fields slowly adapting Meissner's corpuscles 1/10 size of Pacinians much smaller rf's rapidly adapting vibration - 50 Hz Merkel's disks nerve terminal + flattened epithelial cell which makes synapse onto nerve terminals. Epithelial cell may be mechanically sensitive. small rf's slowly adapting Krause end bulbs junctions of dry skin & mucous membrane Hair follicle receptors Nociception: (pain) Free nerve endings Thermoreceptors cold receptors tuned for low skin temperatures (~25 deg C) warm receptors tuned for warm skin temperatures (~43 deg C) Proprioception Latin: proprius = "ones' own" Sensation of one's own body's position & movement Receptors= muscle spindles measure length & rate of muscle stretch Golgi tendon organs gauge force via. tension in tendon Misc. receptors in joint connective tissue Most = rapidly adapting => better for moving joint, worse for resting position Central Somatosensory Pathways: peripheral nerves => dorsal root ganglion ascend in spinal cord sorted by submodality: dorsal column/medial lemniscal pathway touch & vibration, limb proprioception spinothalamic pathway pain & temperature => Nucleus VP of thalamus (ventral posterior) => S1 - primary somatic sensory cortex Neurons have receptive fields on the body surface somatotopy cortical magnification (16.4) fingers, face, lips, genitals >> back, elbow, leg, etc. (analogous to magnification of fovea in visual system; also sometimes see magnification for auditory frequencies; esp. bats - doppler shift) magnification = proportional to density of peripheral receptors Columns = 1 class of sensory receptors / column Perception: Lots of receptor types, but no clean correspondence between receptor type & perception Localization of tactile stimuli accuracy of ability to localize stimuli varies with location on the body surface 2 point threshold = measure of localization ability touch skin with 1 point or 2 points - can you tell the difference? if 2 points are close, can't tell the difference between 1 and 2 separation varies with location on body surface e.g. thumb: 4 mm leg = about 48 mm Thresholds differ for males & females 16.7, 16.8 Pain most pain producing stimuli = potentially damaging e.g. intense thermal, sound, light, chemical & electrical stimulation pain = important for survival patients with insensitivity to pain incur serious skin injuries e.g. leprosy (Hansen's disease), though not specific to pain, results in a loss of pain and other tactile input. Injuries to extremities => gangrene, necrosis Some patients have anomalous disorders that make them unable to feel pain, though other skin senses = intact outcome => failure to protect body from injury usually leads to early death e.g. failure to shift weight, roll over at night => joint decay => infection => death Masking pain can be masked by simultaneous intense stimulation , not painful e.g. rubbing, scratching an itch Phantom limb story: When an area of cortex ceases to be responsive to input from one place and becomes responsive to input from another place on the body, there must be corresponding changes in subsequent areas -- the "LABEL" on the line must be changed every where, or it doesn't make sense. patients with amputation of limbs often continue to be able to "feel" their limbs. Turns out, input from other regions of the body surface are interpreted as being on the phantom limb. (Ramachandran story), can mask pain in the phantom limb Neural basis of perception Involvement of S1 inperception: Map of body surface is plastic: Merzenich experiments -map hand region of cortex -amputate or denervate 1 digit -remap cortex => area previously corresponding to that finger now = responsive to input from neighboring fingers Map = subject to modification based on experience - map hand region train monkey on tactile discrimination task - remap hand region trained finger => expanded cortical representation = possible basis for perceptual learning? microstimulation in S1: Romo et al: trained monkeys to perform a flutter frequency discrimination task then, replaced one flutter stimulus with microstimulation in S1 at appropriate somatotopic location => monkeys could compare stimulation & mechanical stimuli & perform correctly i.e. appropriate stimulation in S1 = sufficiently realistic that it can substitute for an actual tactile stimulus!