Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
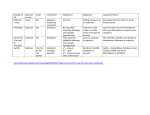
Monitoring treatment and changing therapy Monitoring treatment Patients on ART need close monitoring to assess: Adherence to the prescribed regimen Tolerance and side effects of the medications Efficacy of treatment Monitoring of therapy should be done by both clinical and laboratory assessments CLINICAL MONITORING The frequency of visits for clinical monitoring should be as follows: • The first visit should take place 2 weeks after initiating therapy. This appointment should focus on ensuring that the medicines are being correctly taken and stored. Any side effect should be noted and addressed accordingly. • Subsequent visits should be done monthly if the patient is stable and the focus should be on assessing the patient’s clinical progress and checking for any side effects of the drugs. • After 6 months, if the patient is compliant and clinically stable, appointments may be spaced at 2 to 3 months intervals. At each visit: Plot the patients weight and note the trend. Determine the patient’s physical condition. Address ongoing medical problems including possibility of failure of treatment through the development of new OI. Treat intercurrent infections Check drug dosages. The patients should be given medicines to last for 1month even when the clinic appointments are less frequent. Adherence counseling should be done at each visit. Laboratory monitoring Certain laboratory tests are recommended for assessing response to treatment and also to monitor toxicity. For proper monitoring of efficacy of treatment, CD 4 counts and viral load where available are ideal tests to be done. CD 4+ lymphocyte counts These are a type of lymphocytes, which play an important role in the immune system. HIV-1 infections target these cells resulting in their death and even of those uninfected CD 4 lymphocytes. The CD 4 cell count is a laboratory marker of the strength of ones immune system. Normal count in adults ranges from 500-1800 cells per cubic millimeter of volume Viral Load Viral burden in peripheral blood can be determined by using quantitative HIV RNA assays. During the period of primary infection in adults HIV RNA copies initially rise to high levels. Coincident with the body’s humoral and cell-mediated immune response, RNA levels decline. Patients with lower HIV copies have slower disease progression and improved survival compared with those with high HIV RNA copies. On the basis of such data, recommendations for use of HIV RNA copies in deciding to initiate and change therapy in infected adults have been developed Resistance testing Other laboratory tests are recommended mainly for monitoring drug toxicities and are therefore recommended as baseline before ARVs are instituted. These tests should be available on site or by transportation of specimens to a local reference laboratory. The include: Complete blood count (CBC) ALT/SGPT Creatinine Pregnancy test for all women of child bearing age Fasting lipid profile if Protease inhibitors are to be used Follow-up labs ALT/AST after 1-2 months of treatment when NNRTIs are used for. If normal, repeat the test at 6 months interval or earlier if clinically indicated. CBC after 1 month if Zidovudine is used for treatment. If normal, repeat these tests at 6 months interval Fasting lipids annually if a patient is on protease inhibitors. Evaluation for pregnancy for women of children bearing age and pregnancy tests done when indicated. Repeat CD4 count (where available) at 6 months interval. Viral load (where available) should be done at baseline and then yearly and/or when resistance is suspected SUMMARY TABLE TEST Baseline I month 6 months 12 months 18 months 24 months HIV X CBC X X X X X X AST/ALT X X X X X X Creatinine X X X Fasting lipids X X X Pregnancy test X CD4 X Viral load X1 X1 X1 X1 X1 X X X X ADHERENCE MONITORING Patients should have adherence counseling and assessment at each clinical encounter. Measurement of adherence is imperfect and currently lacks established standards. However, some tools that a can be used include; patient self-reporting, diary cards, medication checks (pill counts), and other improvised measures. HIV viral suppression, reduced rates of resistance and improved survival have been correlated with high rates of adherence to antiretroviral therapy. Greater than 95% adherence is needed to achieve good virological response and to prevent the emergence of viral resistance. For a patient taking medication twice a day, missing more than 1 dose implies <95 adherences. Reason for non-adherence Just forgetting Side effects Complexity of regimens Pill burden Denial of need for treatment CHANGING THERAPY Indications for changing therapy Treatment failure Treatment intolerance Drug interaction (e.g. occurrence of active tuberculosis and or pregnancy) Interruption of drug supply Cost of treatment Treatment failure Antiretroviral treatment failure can be defined as a sub optimal response to therapy. Treatment failure can be clinical, immunological and or virological. Clinical failure Development of new opportunistic infection, wasting, or dementia or failure to resolve pretreatment opportunistic infections when the drugs have been given for at least six months to induce a protective immune system restoration. This needs to be differentiated from an immune reconstitution syndrome, which can be seen within the first eight weeks after the institution of therapy, if a sub clinical infection is present at the time. Although management of immune reconstitution syndromes can be difficult, changing the antiretroviral regimen in these circumstances is not indicated. Immunological failure Failure to significantly increase CD4 count or a persistent decline in CD4 count after a period of immune reconstitution. Virological failure Failure to reduce the viral load to < 400 copies/ml after 24 weeks or <50 copies/ml by 48 weeks of treatment; or failure to reduce the viral load by at least 2 to 2.5 log 10 or a persistent increase in viral load following a period of adequate suppression Despite a good clinical and immunological response, viral resistance will occur in the absence of complete viral suppression. However since viral load measurement are not readily available at the moment many clinicians delay to change therapy unless there are signs of clinical or imunological progression Causes of treatment failure Non-adherance to treatment Viral resistance to one or more drugs Impaired drug absorption Altered drug pharmacology; Interaction with other drugs Factors that increase the risk of treatment failure Prior antiretroviral therapy Very sick patient with very low CD4 counts or high viral load at the time of initiating therapy Poor clinic attendance record Side effects or disease progression Disease processes like intractable vomiting and diarrhea. Considerations for changing a failing regimen As with the initiation of antiretroviral therapy, the decision to change regimens should be approached with careful consideration of several complex factors. Issues to consider when introducing second line therapy include: Do not rush into second line therapy When changing therapy, determine whether poor adherence was responsible for the failure; if its not possible to improve adherence, attempt directly observed therapy with a health worker, family member or a friend If the patient is adherent, assume that resistance has developed and change therapy. The new therapy should include at least three new drugs. Optimally and when possible, the regimen should be changed entirely to drugs that have not been taken previously. With triple combinations of drugs, at least two drugs preferably three drugs should be selected that are not subject to anticipated cross resistance to drugs given previously; this is based on current understanding of strategies to prevent drug resistance When changing therapy review all other medication for possible drug interaction Viral resistance to antiretroviral drugs is important but not the only, reason for treatment failure. Genetically distinct viral mutants emerge in HIV related individual over time after initial infection. Viruses with single drug resistance mutations exist even prior to therapy Changing treatment due to toxicity Treatment may be changed because of adverse events. Adverse events are gross clinical or biochemical abnormalities that may arise from infections, ART, or other drugs and treatment Establish whether the adverse event is due to ARV or to other medication. Not all problems that arise during treatment result from ARV drugs therefore, consider other disease processes e.g. consider isoniazid as a cause of peripheral neuropathy in a patient on ARV drugs taking anti TB drugs. If there is a need to discontinue ARV, it is advisable to discontinue all ARV drugs simultaneously rather than to continue with one or two drugs alone in order to prevent the emergence of drug resistance • Continue ARV if there are grade 1 or 2 reactions (Appendix); single drug substitutions may occasionally be necessary • Treatment should be stopped if grade 3 or 4 reactions occur. Manage the medical event; then reintroduce ARV drugs using a modified regimen In the setting of good therapeutic response, the development of a clearly definable toxicity permits single drug substitutions without compromising the overall regimen. Table showing showing common side effects and what to change into incase of toxicity Drug interactions -Patients on with HIV are often on other medications that interact with ARVs e.g. TB medication. ARV drugs should be deferred in a patients on TB treatment during the intensive phase when on Rifampicin. However, Efavirenz may be substituted for Nevirapine in a patient who is already on ARVs or to whom ARVs are indicated while on Rifampicin based TB treatment. - Efavirenz should not be used in pregnancy especially in the first trimester. -Oral contraceptives are unreliable with NVP/EFV and PI and so there's need to provide alternative /added contraceptive method -Certain ARV drugs compete for the same site and should never be used together Minimizing drug interaction • Ask at each visit what other medication patient is taking. • Educate patient to consult before taking any medicine and to avoid over counter pills • Avoid drugs which interact wherever possible Discontinuation of therapy Once a patient is on ARV he should continue with treatment without interruption, for life. However, under exceptional circumstances it may be necessary to discontinue ARV. Such circumstances include -extremely poor adherence, -serious drug toxicities, -intervening illnesses that precludes oral therapy - cases where the administration of medication is repeatedly interrupted. Continuing sub optimal ARV will lead to emergence of viral resistance. Consider discontinuation only after exploring all potentially corrective measures, including intensive counseling, additional caregiver education and family support. RESISTANCE TESTING In the majority of patients who have never received ARV, the wild type, or non-mutant virus predominates. During therapy the disappearance or suppression of wild-type virus creates the environment in which the mutant virus can become the dominant species. The degree of suppression provided by a treatment regime is therefore, a critical factor in the emergence of HIV drug resistance. Resistance assays may assist clinicians in individualizing initial as well as subsequent antiretroviral treatment regimens for their patients. Resistance testing, where available, is recommended for persons on anti-retroviral treatment whose viral load suppression is sub optimal or viral load is increasing and CD4 cell count is declining. Many studies in patients on treatment have shown strong associations between the presence of drug resistance and failure of the antiretroviral therapy. There are mainly 2 types of resistance testing which unfortunately are not yet available in Kenya. Genotypic Assays These detect drug resistance mutations that are present in the relevant viral genes. They may involve sequencing of the entire reverse transcriptase and protease genes while others go for selected mutations that are known to confer drug resistance. Phenotypic Assays These assays measure the ability of viruses to grow in various concentrations of antiretroviral drugs. They are more expensive and time consuming to perform. Both genotyping and phenotyping assays are limited due to the lack of uniform quality assurance for all available assays, relative high cost and insensitivity for minor viral species. In general, resistance testing may be useful in the setting of virological failure of antiretroviral therapy or in acute HIV infection.