Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Heart failure wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Drug-eluting stent wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
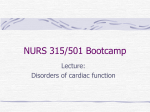
Advances in Vein Therapies Coronary Sinus Anatomy: Ajmer Working Group Classification R.K. Gokhroo, MD, DM, Devendra Singh Bisht, MD, DM, Deepak Padmanabhan, MD, DM, Sajal Gupta, MD, DM tools for common disorders like heart failure has made understanding the coronary sinus (CS) anatomy necessary.8-10 We made an attempt to classify CS anatomy depending upon the size, branching pattern, location of posterolateral vein (PLV), and other parameters. This classification is intended to guide the cardiologist for successful cannulation of the CS and LV lead. Methods In this single-center, non-randomized, observational study, we analyzed the levophase angiograms of 100 patients undergoing routine coronary angiography in the right anterior oblique (RAO) view, and classified these observations on the basis of predetermined parameters; a working classification was produced for the ease of the operator and to predict the bottlenecks of the procedure. All patients gave written informed consent. Patients allergic to radiographic contrast agent were excluded. Coronary angiography. Coronary angiography was performed with Judkins technique via the radial route using a 5 Fr TIG catheter. Venograms were analyzed in the levophase after injection of contrast in the coronary artery ostia. Coronary sinus visualization was observed 8-12 cycles after contrast injection. A non-ionic contrast agent with low osmolarity was used. Terminology and coronary venous anatomy. We used the same terminology as used in previous studies to identify the coronary veins.11-13 The myocardium drains mainly by two groups of veins: the tributaries of the greater and smaller cardiac veins, or the Thebesian veins. The main vein of the greater venous system is the CS, which runs in the posterior aspect of the coronary groove. The anterior wall of the left ventricle and the interventricular septum are drained by branches of the anterior interventricular (AIV) vein, known as the great cardiac vein on the annulus.14-16 The course of the anterior interventricular vein is similar to the adjacent left anterior descending artery in the interventricular groove. In a study using electron-beam computed tomography (CT), the anterior interventricular vein was visualized in up to 100% of subjects scanned.17 In addition, the diameter of the anterior interventricular vein was seen to be similar to the neighboring artery for the length of its course. The great cardiac vein in turn joins the main posterior lateral vein to form the CS. Other major tributaries entering the CS include the inferior left ventricular vein and the middle cardiac vein (MCV), which originates close to the apex of the heart and follows the posterior interventricular groove toward the base. Usually, the MCV drains into the CS close to its ostium in the right atrium. The atrial myocardium also drains into the CS via the various atrial veins and the vein of Marshall. The vein of Marshall is a remnant of the left superior vena cava; it runs along the posterior aspect of the left C . 4 se 01 lU 2 na MP so H er ht r P rig Fo opy Abstract: Background. Coronary sinus (CS) anatomy is a major predictor of successful implantation of left ventricular (LV) lead and procedural outcome. We therefore made an attempt to look at the CS anatomy and possible feasibility to classify them into categories depending upon their size, branching pattern, location of posterolateral vein (PLV), and other parameters in order to guide the cardiologist for successful cannulation of the CS and LV lead implantation. Methods. We analyzed the levophase angiograms of patients (n = 100) undergoing routine coronary angiography in the right anterior oblique view. We have made an attempt to classify these observations on the basis of predetermined parameters and a working classification was brought out for the ease of the operator and to predict the bottlenecks of the procedure. Observations. On the basis of predetermined parameters, venograms obtained from 100 patients were analyzed and findings were divided into three groups depending upon the ease of cannulation of posterolateral vein for LV lead placement. These 3 groups were further classified as type I, type II, and type III coronary sinuses. Conclusions. This observational study proposes a new anatomical working classification for CS for purposes of successful LV lead placement and optimal operative success. J INVASIVE CARDIOL 2014;26(2):71-74 Key words: coronary sinus, cardiac resynchronization therapy, angiography The coronary venous system is increasingly used for biventricular pacing in patients with chronic refractory heart failure. The present study investigated the structure of the coronary veins, and assessed the availability of veins for possible left ventricular (LV) lead placement. A further attempt to classify the coronary venous anatomy on the basis of successful left ventricular lead implantation was made. Background. The coronary venous system is used for various electrophysiological purposes. Cardiac resynchronization therapy (CRT) incorporating an LV lead may profoundly improve the condition of patients with severe heart failure.1,2 The coronary venous system has also been used for various electrophysiological procedures, eg, arrhythmia ablation,3 electroanatomical mapping,4 and implantation of various cardiac devices.5-7 Historically, cardiac vascular studies have focused mainly on the coronary artery circulation. The advent of advanced invasive and interventional cardiac treatment and management From the Department of Cardiology, Institute of Cardiology, JLN Medical College & Associated Group of Hospitals, Ajmer, India. Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein. Manuscript submitted July 1, 2013, provisional acceptance given August 1, 2013, final version accepted August 6, 2013. Address for correspondence: Devendra Singh Bisht, MD, DM, Postgraduate Department of Cardiology, JLN Medical College & Associated Group of Hospitals, Ajmer 305 001, Rajasthan (India). Email: [email protected] Vol. 26, No. 2, February 2014 71 GOKHROO, et al. C . 4 se 01 lU 2 na MP so H er ht r P rig Fo opy Figure 1. Hypothetical representation of three types of coronary sinus in right anterior oblique view depending upon predefined parameters and angiographic findings of patients analyzed. PLV); and (9) other findings such as valves, CS diverticula, muscle sleeves in CS, and obstructed CS. Since the sole purpose of the present study was to assess the potential availability and ease of cannulation of posterolateral veins for placement of LV lead of CRT device, predetermined parameters were chosen keeping the above fact Figure 2. Coronary venogram analysis in right anterior oblique view from three patients showing 3 types of coro- in mind. nary sinus. Venograms show that LV lead placement is easiest in type I and most difficult in type III coronary sinus. Observations. On the basis of predetermined paramatrium and is formed by the junction of the great cardiac vein eters, venograms obtained from 100 patients were analyzed and and the posterolateral vein.18 The right atrium and the posterior findings were divided into three groups (Table 1) depending and posterolateral portions of the right ventricle are drained by upon the ease of cannulation of posterolateral vein for LV lead the small cardiac vein into the CS at the ostium of the right placement. These 3 groups were further classified as type I, type atrium. The smaller cardiac venous system is the Thebesian ve- II, or type III coronary sinuses (Figures 1 and 2). Our working nous network. This system is responsible for draining the inner experience suggests that type I coronary sinus has the easiest layers of the myocardium of the right ventricular venous system cannulation rate, whereas type III is the most difficult. and portions of the interventricular septum directly into the right ventricle via orifices that are often 0.5 mm in diameter. Discussion Venogram analysis. Four experienced cardiologists anaThe high degree of variability in coronary venous anatomy lyzed the venogram under the following predetermined param- makes it important to have a uniform segmental classification eters: (1)diameter of CS ostium; (2) diameter of posterolateral system for cannulating these vessels. It will be helpful for the vein; (3)mean diameter of CS before posterolateral vein; (4) electrophysiologist to classify coronary sinus tributaries by their number of lateral vein branches; (5) tortuosity of coronary ve- epicardial location in addition to their anatomic classification. nous system between optimal lead implantation site (usually Further approaches to epicardial lead placement may inPLV) and CS ostium; angle between axis of body of CS and hori- volve a non-invasive definition of the coronary venous anatozontal plane passing through the ostium of the CS; (7) tortuosity my prior to procedure, followed by more selective angiographic of the vein that is the ideal site for lead implantation (usually techniques to enable better definition of the coronary venous PLV); (8) distance between the CS ostium and the ostium of anatomy for LV lead placement. Recognition of the venous the vein that is the ideal site for implantation of LV lead (usually tributaries in terms of their distribution, angulation, tortuosity, 72 The Journal of Invasive Cardiology® Coronary Sinus Anatomy: Ajmer Working Group Classification Table 1. Findings on venogram analysis. Parameters (n = 100) Type I Type II Size of ostium >10 mm (30%) 5-10 mm (63%) <5 mm (7%) Mean size of CS before PLV >10 mm (8%) 5-10 mm (67%) <5 mm (25%) Mean size of PLV >4 mm (7%) 2-4 mm (53%) <2 mm (40%) Ratio of mean CS size/PLV size <2 (40%) 2-4 (53%) >4 (7%) Total number of lateral branches >2 (27%) 2 (39%) <2 (34%) Total number of veins between anterior interventricular vein and middle cardiac vein >2 (52%) 2 (36%) <2 (12%) 2 curves <75° or 1 curve >75°(68%) 2 curves >75° (31%) 3 curves >75° (1%) Angle between axis of body of CS and horizontal plane passing through the ostium of the CS <45° (28%) 45°-90° (66%) >90° (6%) Tortuosity of the vein that is the ideal site for lead implantation Absent/<2 curves (65%) 2 curves (30%) >2 curves (5%) <10 mm (0%) 11-40 mm (71%) >40 mm (29%) no valves (51%) valves in the anterior/middle or posterior veins (22%) Thebesian valve and valve of Vieussens (27%) separate opening of the posterior vein and middle cardiac vein (67%) common opening of posterior vein and middle cardiac vein (33%) obstructed CS (3%) muscle Sleeve in CS (33%) CS diverticula (0%) Tortuosity between optimal lead implantation site and CS ostium C Valves . 4 se 01 lU 2 na MP so H er ht r P rig Fo opy Distance between the CS ostium and the ostium of the vein that is the ideal site for implantation of LV lead Other findings Type III Values in parentheses signify the number or percentage of patients having the same observation. It is evident that type II is the most common among the patients studied. CS = coronary sinus; PLV = posterolateral vein. and dimensions will enable the development of lead positioning tailored to each individual patient. We therefore proposed a new anatomical working classification for CS for purposes of successful LV lead placement and optimal operative success (Table 1). The venous drainage of the left ventricle is variable and typically gives multiple options for the implanter.19,20 The posterolateral vein is the ideal vein to attempt cannulation because it drains the free wall of the left ventricle; however, in cases of difficult CS anatomy, lateral tributaries of anterior interventricular vein, posterior ventricular vein, or middle cardiac veins can be used to pace the LV free wall.21 The MCV can be specifically targeted for placing an LV lead.21 Although the MCV lies in the posterior interventricular septum, various branches/tributaries drain the lateral wall toward this vein. Being perpendicular to the main access of the CS, cannulation is not straightforward. Once entered, the pacing lead can then be placed in this vein and carefully maneuvered to the LV free wall.22-24 Often, the posterior vein can be cannulated. Sometimes, a common ostium for the posterior and MCV occurs and may need specific cannulation either for placement of pacing leads or ablation of posterior epicardial accessory pathways.21 Sixty-four slice or dual-source computed tomography may be a valuable tool to evaluate coronary venous anatomy prior to invasive procedures. Performing multidetector computed Vol. 26, No. 2, February 2014 tomography (MDCT) has been recommended to non-invasively evaluate the coronary vein map before attempting biventricular pacemaker implantation.25 The venous diameters, courses, and relationships to other cardiac structures may be examined in detail using multiplanar reconstructions and volume-rendering technique images. The main problem encountered during evaluation of coronary venous system using electrocardiographic-gated MDCT is to select the optimal phase for reconstruction.26,27 Further imaging of the coronary venous system using routine coronary CT angiography protocol may not always be feasible in heart failure patients due to heightened heart rate, various cardiac arrhythmias, and an inability to hold breath because of respiratory symptoms. It is also possible to evaluate the coronary venous system using electron-beam CT. However, many patients may not be adequately assessed by this modality because of suboptimal image quality and not all parts of the heart come under examination.28,29 Study limitations. The transverse diameter of the epicardial veins remains constant during systole and diastole, with flow occurring as a bolus during each cardiac cycle. Therefore, uniform opacification of the entire cardiac venous system including tributaries is difficult with a single bolus of contrast delivered at the proximal end.30 Further single-frame analysis of coronary angiogram doesn’t provide sufficient information about coronary sinus anatomy. 73 GOKHROO, et al. C Conclusion The presence, diameter, angulation, and tortuosity of coronary veins determine their acceptability for the placement of an LV lead in a predetermined location. Despite the considerable variability of the coronary venous system among patients, a lateral vein for lead implantation is available in the majority of patients. Furthermore, this classification system attempts not to supplant, but rather adds information to the conventional coronary venous anatomy, which is of particular relevance to the electrophysiologist. References 1. Daubert CJ, Ritter P, LeBreton H, et al. permanent left ventricular pacing with transvenous leads inserted into the coronary veins. Pacing Clin Electrophysiol. 1998;21(1 Pt 2):239-245. 2. Auricchio A, Stellbrink Ch, Sack S, et al. Transvenous biventricular pacing for heart failure: can the obstacles be overcome? Am J Cardiol. 1999; 83(5B):136D-142D. 3. Stellbrink C, Diem B, Schauerte P, et al. Transcoronary venous radiofrequency catheter 74 ablation of ventricular tachycardia. J Cardiovasc Electrophysiol. 1997;8(8):916-921. 4. Cappato R, Schlüter M, Weiss C, et al. Mapping of the coronary sinus and great cardiac vein using a 2-french electrode catheter and a right femoral approach. J Cardiovasc Electrophysiol. 1997;8(4):371-376. 5. Roberts PR, Urban JF, Betts T, et al. Reduction in defibrillation threshold using an auxiliary shock delivered in the middle cardiac vein. Pacing Clin Electrophysiol. 2000;23(8):1278-1282. 6. Kenknight BH, Walker RG, Ideker RE. Marked reduction of ventricular defibrillation threshold by application of an auxiliary shock to a catheter electrode in the left posterior coronary vein of dogs. J Cardiovasc Electrophysiol. 2000;11(8):900-906. 7. Butter C, Meisel E, Engelmann L, et al. Human experience with transvenous biventricular defibrillation using an electrode in a left ventricular vein. Pacing Clin Electrophysiol. 2002;25(3):324-331. 8. Abraham W, Leon A, Hannon C, Prather W, Fieberg A. Results of the InSync III Marquis clinical trial (Abstr). Heart Rhythm. 2005;2:S65. 9. Abraham WT, Fisher WG, Smith AL, et al. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002;346(24):1845-1853. 10.Cleland JG, Daubert JC, Erdmann E, et al. The CARE-HF study (CArdiac REsynchronisation in Heart Failure study): rationale, design and end-points. Eur J Heart Fail. 2001;3(4):481-489. 11. Schumacher B, Tebbenjohanns J, Pfeiffer D, et al. Prospective study of retrograde coronary venography in patients with posteroseptal and left sided accessory atrioventricular pathways. Am Heart J. 1995;130(5):1031-1039. 12. Gilard M, Mansourati J, Etienne Y, et al. Angiographic anatomy of the coronary sinus and its tributaries. Pacing Clin Electrophysiol. 1998;21(11 pt 2):2280-2284. 13. Gensini GG, Giorgi S, Coskun O. Anatomy of the coronary circulation in living man: coronary venography. Circulation. 1965;31:778-784. 14. Grzybiak M. Morphology of the CS and contemporary cardiac electrophysiology. Folia Morphol (Warsz). 1996;55(4):272-273. 15. D’Cruz IA, Shala MB, Johns C. Echocardiography of the CS in adults. Clin Cardiol. 2000;23(3):149-154. 16. Ortale JR, Gabriel EA, Iost C, Marquez CQ. The anatomy of the CS and its tributaries. Surg Radiol Anat. 2001;23(1):15-21. 17. Schaffler GJ, Groell R, Peichel KH, Rienmuller R. Imaging the coronary venous drainage system using electron-beam CT. Surg Radiol Anat. 2000;22(1):35-39. 18. Cendrowska-Pinkosz M, Urbanowicz Z. Analysis of the course and the ostium of the oblique vein of the left atrium. Folia Morphol (Warsz). 2000;59(3):163-166. 19. Ruengsakulrach P, Buxton BF. Anatomic and hemodynamic considerations influencing the efficiency of retrograde cardioplegia. Ann Thorac Surg. 2001;71(4):1389-1395. 20.Sethna DH, Moffitt EA. An appreciation of the coronary circulation. Anesth Analg. 1986;65(3):294-305. 21. Habib A, Lachman N, Christensen KN, Asirvatham SJ. The anatomy of the coronary sinus venous system for the cardiac electrophysiologist. Europace. 2009;(11 Suppl 5):v15-v21. 22. Schaffler GJ, Groell R, Peichel KH, Rienmuller R. Imaging the coronary venous drainage system using electron-beam CT. Surg Radiol Anat. 2000;22(1):35-39. 23. Asirvatham S. Anatomy of the CS. In: Cheuk-Man Y, ed. Cardiac Resynchronization Therapy. Oxford: Blackwell Publishing, 2006:211-238. 24. Von Lüdinghausen M. Clinical anatomy of cardiac veins, Vv. cardiacae. Surg Radiol Anat. 1987;9(2):159-168. 25. Hendel RC, Patel MR, Kramer CM, et al. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/ SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006;48(7):1475-1497. 26. Mlynarski R, Sosnowski M, Wlodyka A, Kargul W, Tendera M. A user friendly method of cardiac venous system visualization in 64-slice computed tomography. Pacing Clin Electrophysiol. 2009;32(3):323-329. 27. Mlynarski R, Sosnowski M, Wlodyka A, Chromik K, Kargul W, Tendera M. Optimal image reconstruction intervals for noninvasive visualization of the cardiac venous system with a 64-slice computed tomography. Int J Cardiovasc Imag. 2009;25(6):635-641. 28. Mao S, Shinbane JS, Girsky MJ, et al. Coronary venous imaging with electron beam computed tomographic angiography: three-dimensional mapping and relationship with coronary arteries. Am Heart J. 2005;150(2):315-322. 29. Schaffler GJ, Groell R, Peichel KH, et al. Imaging the coronary venous drainage system using electron-beam CT. Surg Radiol Anat. 2000;22(1):35-39. 30. Hodgson EJ, Armour JA, Klassen GA. Functional anatomy of the epicardial coronary veins. Can J Cardiol. 1993;9(9):821-828. 31. Gilard M, Mansourati J, Etienne Y, et al. Angiographic anatomy of the coronary sinus and its tributaries. Pacing Clin Electrophysiol. 1998;21(11 Pt 2):2280-2284. 32. Daoud EG, Kalbfleisch SJ, Hummel JD, et al. Implantation techniques and chronic lead parameters of biventricular pacing dual-chamber defibrillators. J Cardiovasc Electrophysiol. 2002;13(10):964-970. . 4 se 01 lU 2 na MP so H er ht r P rig Fo opy We did not perform conventional balloon occlusion venography31 because this may lead to raised backpressure, which may cause distension of the venous system and values may get overestimated. Furthermore, unlike anterograde coronary arteriography, balloon occlusion coronary venography is often limited by the vigorous backwash of the injected contrast, which impairs the ability to define the detailed anatomy of the tributaries and collateral circulation. We analyzed the angiograms in only the right anterior oblique view to avoid excessive contrast and radiation exposure, whereas coronary venous angiography should be performed in at least two different views with the necessary caudal or cranial angulations to separate the branches and display the course of the main branches, which is key to the segmental approach. We know that a left anterior oblique view is necessary to perfectly define the lateral position of a CS vein. All of our patients are not suffering from cardiomyopathy, whereas patients receiving cardiac resynchronization therapy devices have an underlying cardiomyopathy and may have had extensive remodeling and rotation of the heart. Hence, subselective angiography of the main branches is often important to clearly define the pattern of distribution of the second- and third-order tributaries for optimal lead placement. We have classified coronary sinus into three categories, but an individual CS could have characteristics of all three types, eg, a type I ostium, a type II mean size of the PLV, and a type III number of lateral branches, etc. The success rate for placement of a transvenous cardiac resynchronization system has ranged from approximately 88% to 92% in clinical trials.32 We do not consider type III coronary sinus to be a contraindication to device implantation; however; we consider that in type III coronary sinus, the technique of the procedure is challenging and cannulation of the coronary sinus and subsequent manipulation within its tributaries remain difficult despite substantial improvements in hardwares. Dissection of the coronary sinus is one of the major complications of type III coronary sinus, especially for the beginner operators. Currently, the data from our center to justify this hypothesis are limited and further research is needed for validation. The Journal of Invasive Cardiology®