Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
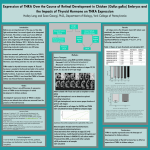
Thyroid Nodules and Thyroid Cancer Dr. Boyd Lee Otolaryngology – Head and Neck Surgery Memorial University Anatomy Anatomy • 2 lateral lobes connected by isthmus • Pyramidal lobe 50% • Isthmus lies over 2nd – 3rd tracheal ring Anatomy • Blood supply – Superior and Inferior thyroid a. – Superior, middle, and inferior thyroid v. Anatomy • Lymphatic drainage – Prelaryngeal (delphian) node – Pretracheal nodes – Paratracheal nodes – Lateral neck nodes Thyroid Lymphatics Anatomy • Innervation – Parasympathetic via vagus – Sympathetic via cervical sympathetic chain Anatomy • Recurrent Laryngeal nerves – Lie in Tracheoesophageal grooves adjacent to thyroid – Branches of Vagus n. – Left loops around aortic arch – Right loops around right subclavian a. – Innervates intrinsic muscles of larynx except cricothyroid m. Anatomy • Parathyroid glands – Paired superior and inferior parathyroid glands on posterior aspect of thyroid within thyroid capsule Physiology • Endocrine gland • Follicular cells produce T4 and T3 • Parafollicular cells (C cells) produce calcitonin Thyroid Disorders • Disorders of function – Hypothyroidism – Hyperthyroidism – Autoimmune • Disorders of anatomy – Thyroid nodules • Cysts • Adenomas • Carcinomas – Goiter Thyroid Nodules • “Discrete lesion within the thyroid gland that is radiologically distinct from the surrounding thyroid parenchyma.” • Not all palpable lesions correspond to a radiologically distinct abnormality • Presence of a nodule(s) in the thyroid does not necessarily affect function of the gland Thyroid Nodule Thyroid Nodules • Palpable thyroid nodules – 5% of women – 1% of males • US detected nodules – 19-67% randomly selected individuals – Higher incidence in women and the elderly • Generally, only nodules >1 cm need to be investigated unless other factors or SSx present Thyroid Nodules • Only 6% of 1 cm nodules are palpable • Only 50% of 1-2cm nodules are palpable • Even 50-60% of >2 cm nodules are not detected clinically • Non-palpable nodules carry same risk of malignancy as palpable nodules • Factors affecting the palpability of nodules – Size of nodule – Thickness of neck – Position of the nodule (posterior, inferior, retro-sternal) – Experience of the examiner Thyroid Nodules • 5-15% of thyroid nodules are malignant • Depends on: – – – – Age Sex Radiation exposure Family history Thyroid Cancer • Well Differentiated – Papillary (85%) – Follicular (5%) • Poorly Differentiated – Medullary (5%) – Anaplastic • Other – Lymphoma – Sarcoma – Metastases Thyroid Cancer • Thyroid Cancer is one of 2 cancers that has an increasing incidence • 3.6/100 000 in 1973 • 8.7/100 000 in 2002 • Increase is almost entirely due to papillary thyroid ca (PTC) • Increase may be partly due to better detection • May also be secondary to increased radiation esposure Thyroid Nodule Workup • Thorough History and Physical Thyroid Nodule Workup • History – Childhood neck radiation or ionizing radiation exposure from fallout in childhood – Total body irradiation for BMT or Hodgkins – FHx of Thyroid Ca, MEN, Cowden, Gardner, or Werner syndromes. – Rapid growth – Hoarseness • Physical – – – – Fixation of nodule Vocal cord paralysis Cervical adenopathy > 1 cm Thyroid Nodule Workup • Thyroid Function studies – Serum TSH – If TSH is subnormal nuclear medicine scan is ordered – No further workup necessary if the nodule is hyperfunctioning (ie hot) Thyroid Nodule Workup • Diagnostic Imaging – Thyroid US should be performed in all patients with known or suspected thyroid nodules Thyroid Nodule Workup • US findings suggesting a benign nodule – Purely cystic – Spongiform nodule • US findings suggesting a malignant nodule – Hypoechogenicity – Increased intranodular vascularity – Irregular infiltrative margins – Microcalcifications – Absent halo – Shape taller than width in transverse dimension Thyroid US Spongiform Nodule Thyroid Cyst Mixed Cyst Papillary Ca Papillary Ca Fine Needle Aspiration Bx • FNA is the most accurate and cost effective method for evaluating thyroid nodules. • US guidance increases sensitivity and specificity of the FNA Thyroid FNA FNA Results • • • • • Benign (5% risk of cancer) Suspicious for Cancer (85% risk of Ca) Cancer (95% risk of Ca) Follicular Lesion Atypical lesion of uncertain significance (515% risk of Ca) • Non-diagnostic Indications for Thyroid Surgery • Cancer (Papillary, Follicular, Medullary) • Suspicion for, or risk of Cancer • Compressive Sx – Dyspnea – Dysphagia • Hyperthyroidism • Cosmesis Pre-op/ Post-op Assessment • Flexible laryngoscopy • US of lateral neck if Papillary Ca to determine presence of lymphadenopathy + FNA Bx of any suspicious nodes Papillary Thyroid Ca • • • • • • Females > males Increased risk from radiation Can be multi-focal Lymphatic spread Role of 131I treatment post -op Excellent prognosis – 97% 5 yr survival – 93% 10 yr survival – Prognosis better in age < 45, females Follicular Thyroid Ca • • • • • Cannot Dx on FNA Dx made on vascular or capsular invasion Hematogenous spread to lungs, bone Role of 131I treatment post -op Very good prognosis – 91% 5 yr survival – 85% 10 yr survival Medullary Thyroid Ca • • • • • • • • Arises from C cells 25% of cases are genetic (MEN 2) RET proto-oncogene Calcitonin and CEA are makers Presents with flushing/diarrhea No role for 131I post op 80% 5 yr survival 75% 10 yr survival Anaplastic Thyroid Ca • Poorly differentiated • Highly aggressive • Can be difficult to distinguish from thyroidal lymphoma • Surgical therapy includes open biopsy & palliative tracheostomy • External beam radiation • Very poor prognosis The Future of Thyroid Surgery Summary • Thyroid nodules are very common • Can be hard to palpate • More commonly diagnosed due to imaging for other reasons (incedentalomas) • Thyroid cancer is increasing • Overall good prognosis compared with other cancers