Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
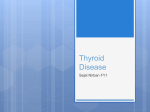
Endocrine Disorders Thyroid Gland Jane E. Binetti DNP MSN RN Thyroid Gland • In the neck, anterior to the trachea • Extremely vascular • Regulated by: ▫ TSH • Produces and secretes ▫ T4 (thyroxine) ▫ T3 (triiodothyronine) ▫ Calcitonin What about Thyroid Gland • Thyroid disorders are the most common of all endocrine issues • Thyroid hormones regulate ▫ Metabolism ▫ Growth and development • Disorders of the thyroid ▫ ▫ ▫ ▫ Goiter Nodules Thyroiditis Hyper/hypo Goiter • Large thyroid gland • Gland is stimulated to grow ▫ Can lead to hyperthyroidism or hypothyroidism ▫ Worldwide, most often due to lack of iodine • In US caused by: ▫ Nodules, or over/under production of hormone ▫ Goitrogens are thyroid inhibiting substances Broccoli, cabbage, kale, cauliflower, mustard, peanuts Lithium, amiodorone, salicylates, sulfonamides More on Goiters • Non toxic Goiters ▫ Enlargement not from inflammation or cancer ▫ Pt has normal thyroid levels • Nodular Goiter ▫ Secrete thyroid hormone without TSH stimulation ▫ Usually benign adenoma • Toxic Nodular Goiter ▫ Toxic because they cause hyperthyroidism ▫ Most frequent after 40 ▫ Common in Grave’s Disease Thyroiditis • Inflammation of thyroid that can cause a goiter • Types ▫ Subacute - viral infections ▫ Acute - bacteria and fungus ▫ Hashimoto’s is autoimmune; tissue is destroyed by antibodies ▫ Silent painless goiter occurs within 6 mo post partum Autoimmune reaction to fetal cells in the mom’s thyroid ? Early Hashimoto’s? Thyroiditis Treatment • Acute or subacute may resolve in weeks or months with no treatment • Antibiotics as necessary for bacterial, even drainage • NSAIDS or steroids for inflammation • Propranolol (Inderal) or atenolol (Tenormin) for cardiac sx • Thyroid hormone for resulting hypothyroidism • Teach compliance with treatment Hyperthyroidism • Over secretion of thyroid hormones ▫ ▫ ▫ ▫ Seen more in women than men 20-40 years old Most common form is Grave’s disease Other causes: thyroiditis, toxic nodular goiter, excess iodine intake, pituitary tumors, thyroid CA ▫ Thyrotoxicosis is acute, severe hyperthyroidism Grave’s Disease • • • • 75 - 80% of hyperthyroidism cases Autoimmune Diffuse large thyroid gland Antibodies attach to TSH receptors, cause over secretion of T3 and T4 • Can remit and exacerbate without tx • Precipitating risk: ▫ iodine, infection, stress, genetic factors, smoking • Can cause thyrotoxicosis • Can degrade the thyroid, lead to hypothyroidism What do you see? • Excess thyroid hormone causes: ▫ ▫ ▫ ▫ ▫ ▫ ▫ ▫ Large gland – goiter Bruit in the gland Exophthalmos Tachycardia, bounding pulse Nervousness, irritability, tremors Flushed skin, heat intolerance Diarrhea, weight loss Fatigue, muscle weakness, edema, osteoporosis Exophthalmos Diagnostics • Thyroid studies ▫ ▫ ▫ ▫ ▫ ▫ TSH – most accurate test of thyroid function Total T4, Free T4 Total T3, Free T3 Thyroid antibodies Thyroid scans, ultrasound Biopsies Diagnostics • • • • TSH levels will be decreased Free T4 levels increased Total T3 and T4 not definitive RAIU – Radioactive Iodine Uptake ▫ Used to differentiate Grave’s from thyroiditis ▫ Grave’s uptake = 35% - 95% ▫ Thyroiditis = < 2% Complications • Thyrotoxicosis (Thyroid Storm) ▫ Life threatening, rare ▫ Abrupt onset -sudden release of thyroid hormones ▫ Precipitated by stress, thyroidectomy, trauma or an acute infection • Symptoms ▫ Extreme fever, tachycardia ▫ Tremors, Seizures ▫ Loss of mental acuity -> Delirium Stupor -> Coma Collaborative Care • Goal is to stop the effects of overproduction ▫ Anti-thyroid medications ▫ Radioactive Iodine therapy ▫ Subtotal or total thyroidectomy • Choice of therapy depends on ▫ Patient age ▫ Severity of disease ▫ Complicating situations More on therapies • Anti-thyroid drugs: ▫ PTU – (propylthiouracil) Inhibits synthesis of thyroid hormones Blocks peripheral conversion of T4 to T3 ▫ Tapazole (methimazole) Improvement in 1-2 weeks, better in 4-8 • 20-40% have spontaneous remission (6-15mo) • Noncompliance is a big issue • Used for Grave’s, in pregnancy, and need for euthyroid before surgery or radiation Anti-Thyroid meds continued • Iodine ▫ Used with other drugs for thyroidectomy prep or thyrotoxic crisis ▫ Inhibits synthesis of T3 and T4 and blocks release ▫ Decreases vascularity in gland ▫ Max effect in 1-2 weeks ▫ Reduced effect long term ▫ SSKI and Lugol’s solution Beta Adrenergic Blockers • Symptomatic relief of thyrotoxicosis • Block sympathetic nervous stimulation • Excess thyroid hormone stimulates B adrenergic receptors • Beta Adrenergics used in conjunction with anti thyroids ▫ Propranolol (Inderal) ▫ Atenolol (Tenormin) for asthmatics and cardiacs Radioactive Iodine Therapy • Treatment of choice in non-pregnant adults • Damages or destroys all thyroid tissue to control secretion of hormones ▫ High incidence of post treatment hypothyroidism • Delayed response requires anti-thyroid drugs and beta adrenergics initially • Radioactivity is low, so done outpatient • Pt Education important!!! Surgical Therapy • Thyroidectomy ▫ Large goiters with compression ▫ Non responsive to medical tx ▫ Cancer • Subtotal ▫ Removes most of gland but not all • Endoscopic ▫ Small incisions to take some gland, or nodes • Prior to surgery meds can make pt euthyroid Post op complications • Hypothyroidism • Damage or removal of parathyroid glands ▫ Causes hypoparathyroidism and hypocalcemia • • • • Hemorrhage Injury to recurrent laryngeal nerve Thyrotoxic crisis Infection Nutritional Therapy • Hyperthyroid state ▫ Hypermetabolic state needs increased caloric intake ▫ Satisfy hunger, prevent catabolic state ▫ High protein, high carbs ▫ Avoid highly seasoned, high fiber foods ▫ No caffeine What do you do? • Hyperthyroidism is treated as outpatient • Acute thyrotoxicosis are admitted to ICU ▫ ▫ ▫ ▫ ▫ ▫ ▫ ▫ Assess your patient! Meds ordered to block thyroid hormone production O2, IVs, watch electrolytes, EKGs Calm, quiet, cool environment Emotional support Eye protection, elevate HOB, skin care Dietary support Pt education Post -op • Assess your patient!! • Semi-Fowlers, post op VS • Laryngeal nerve irritation or damage can lead to spasm and stridor ▫ Can be related to tetany – damage to parathyroids and hypocalcemia ▫ Watch for signs of hypoparthyroidism Assess tingling of extremities and mouth ▫ Chvostek’s and Trousseau’s • Watch bleeding – neck swelling and behind the neck • Hoarse for 3-4 days • Post op pain meds Hypothyroidism • Undersecretion of thyroid hormones ▫ One of most common medical disorders in US 1 in 50 women; 1 in 300 men ▫ Primary from destruction of thyroid or defective synthesis ▫ Secondary from pituitary or hypothalamic disease or dysfunction ▫ Radiation exposure to the neck, family history, women >50 and post-partal • Transient causes: ▫ Thyroiditis ▫ Non-compliance Primary Hypothyroidism • Worldwide caused by lack of iodine in diet • In US most common cause is atrophy of gland ▫ Hashimoto’s thyroiditis ▫ Grave’s disease for long time ▫ Treatment of hyperthyroidism causes hypothyroidism Surgical removal RAI ▫ Drugs Amiodorone (Cordarone) – has iodine Lithium blocks hormone release ▫ Develops in infancy - cretinism What do you see? • Deficiency causes: ▫ Capillary fragility, varied BP, cardiac hypertrophy, anemia, angina, MI ▫ Dyspnea ▫ Decreased appetite, N/V, constipation, wt gain, scaly tongue ▫ Brittle nails, poor turgor, puffy face, pallor, decreased sweating Diagnostics • TSH and free T4 are most often used in conjunction with physical exam • TSH helps determine cause ▫ High TSH = defect in the gland ▫ Low TSH = defect in the hypothalamus or pituitary • After TRH stimulation ▫ Hi TSH = hypothalamus issues ▫ No change = anterior pituitary • TPO AB means cause is autoimmune Complications • Myxedema Coma ▫ ▫ ▫ ▫ Progressive or sudden onset Usually severe long term hypothyroidism Medical Emergency Precipitated by: Infection, medications, exposure to cold, or trauma • Symptoms ▫ Subnormal temp ▫ Hypotension ▫ Hypoventilation • Tx: IV thyroid hormone replacement, VS support Collaborative/Nursing Care • Euthyroid is the goal ▫ Synthroid – levothyroxine Adjusted to pt response and labs Cardiac pts have reduced dose Daily dose taken regularly ▫ Liotrix – 4:1 T4:T3; for pts acutely ill, faster onset • • • • Low calorie diet to aid weight loss Mechanical cardiac /respiratory support prn Assess VS, I/O, wt, mental status Pt education – compliance!