Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacognosy wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Neuropharmacology wikipedia , lookup
Drug design wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug interaction wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Non-specific effect of vaccines wikipedia , lookup
Theralizumab wikipedia , lookup
Psychopharmacology wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
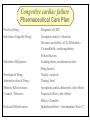
Congestive Heart Failure Dr Ian Coombes Adopted from Duncan McRobbie Principal Clinical Pharmacist (with permission) Signs and Symptoms • • • • • • • • fatigue exertional dyspnoea orthopnoea PND cardiomegaly pitting oedema crackles raised JVP NYHA Classification • NYHA I - no limitation of physical activity • NYHA II- slight limitation • NYHA III - marked limitation • NYHA IV - inability to carry out physical activity Causes • • • • • • acute MI hypertension toxins (alcohol, cytotoxics) viruses/bacteria valve disease cardiomyopathies Prevalence • • • • • 1-2% population 3-5% of those >65 years of age 10% of those >80 years 50% patients die within 2 years of diagnosis 65% of patients with severe CHF die within 1 yr Survival After Initial Diagnosis of HF 100% 50% 0% 3 months 18 months Hospitalisations 74,500 hospital admissions in 2000/2001 Length of stay > 13 days (3x average LOS) 1,000,000 in-patient days Admission rates projected to increase by >50% over the next 25 years Readmission rates as high as 50% over 3 months Readmission - causes Causes of Readmission Arrythmias Infections Frequency (%) 8-28 16-23 Poor compliance Angina Iatrogenic factors Inadequate drug therapy 15-32 14-33 10 17 Inadequate discharge/follow up Failed social support system Erhardt and Cline 1998 (Lancet) 35 21 Signs and Symptoms Symptoms SOA Signs Tachycardia Investigations Chest X-ray SOBOE Fatigue Orthopnoea PND (Paroxysmal nocturnal dyspnoea) Nocturia Increased JVP Oedema Rales Hepatomegaly Echocardiogram Ambulatory ECG Exercise treadmill Cardiac catheter Anorexia Weight loss Cardiomegaly Ascites Classifying Heart Failure – the New York Heart Association method • NYHA I No symptoms with ordinary physical activity (walking and climbing stairs) • NYHA II (mild) Slight limitation of activity with dyspnoea on moderate to severe activity (climbing stairs or walking uphill) • NYHA III (moderate) Marked limitation of activity. Less than ordinary activity causes dyspnoea (restricting walking distance and limiting climbing to one flight of stairs) • NYHA IV (severe) Severe disability, dyspnoea at rest (unable to carry out physical activity without discomfort) Rules of HF Remember symptoms haemodynamics symptoms survival Remember CO=SVxHR BP=TPRxCO Remember Starling’s Law: preload = force of contraction Lapace’s Law: large heart = inefficient Neurohormonal model of Heart Failure – Sympathetic Response afterload cardiac workload arterioconstriction norepinephrine aortic blood flow cardiac output SNS Remember CO = SV x HR Neurohormonal model of Heart Failure – renin-angiotensin-aldosterone afterload preload cardiac workload arterioconstriction Remember Starlings Law remodelling Na+ and H2O retention aldosterone cardiac output Renal blood flow RAS angiotensin venoconstriction Treatment of Heart Failure Remember Survival = drug treatment afterload hydralazine preload cardiac workload diuretics arterioconstriction digoxin norepinephrine aortic blood flow SNS Na+ and H2O retention spironolactone aldosterone cardiac output Renal blood flow RAS B-blockers ACE-I angiotensin naturetic peptides NEP-I nitrates venoconstriction Role of Diuretics • loops most effective • symptomatic relief • Na+ retention • H2O loss • preload ( ventricle filling pressure) • afterload (arterial dilatation) Side effects • dehydration • hypotension • hypokalaemia • hypomagnesaemia • hypouricaemia and gout • non-compliance issues Role of ACE-inhibitors • improves mortality • • • • Side effects (CONSENSUS) • hypotension (6%) better than vasodilator • hyperkalaemia (6%) therapy (VeHFT I and II) • cough (40%) large well conducted • dizziness (50%) trials preload (inhibits effect) • raised serum creatinine (0.2%) afterload (inhibits vasoconstriction) Circulating Renin-Angiotensin System angiotensinogen renin Ang I A C E Ang II AT1/AT2 receptors Potential Role of Angiotensin (1-7) angiotensinogen renin Ang I N E P Ang (1-7) ACE Ang II AT1 AT2 ATx pressor trophic antinatriuretic depressor antitrophic natriuretic depressor antitrophic natriuretic A C E Ang (1-5) Potential Role of Angiotensin (1-7) angiotensinogen ACE inhibitor renin N E P Ang I ACE inhibitor + Ang (1-7) ACE – Ang II AT1 AT2 ATx pressor trophic antinatriuretic depressor antitrophic natriuretic depressor antitrophic natriuretic A C E Ang (1-5) Renin-Angiotensin/Kallikrein-Kinin Systems kininogen angiotensinogen kallikrein renin + bradykinin Ang I ACE kininase II inhibitor icatibant inactive peptides B2 receptor B2 knock-out NO depressor antitrophic cardioprotective ACE – Ang II AT1 AT2 pressor trophic antinatriuretic depressor antitrophic natriuretic Landmark trials with ACE inhibitors in HF Trial n EF% Drug Death Hospitalisation Follow up NNT (death) CONSENSUS 1987 SOLVD-P 1992 SOLVD – T 1991 ATLAS 1997 253 <35% (IV) <35 (I) < 40 (II-III) <35 (II-IV) enalapril 36 vs 50 reduced 1 year 6 enalapril reduced 4 years 104 enalapril trend to reduction 12.3 vs 15.5 reduced 3 years 31 lisinopril no difference reduced 4 years - 4228 2500 3164 Role of ARBs • improves mortality (ELITE I and II / CHARM) • added into conventional therapy (ValHeft / CHARM) • Less s/es Role of Beta blockers • improves mortality (CIBIS 2) • added into conventional therapy • attenuates sympathetic drive (outweighs -ve ionotropic effect) • not all beta-blockers are equivalent (bisoprolol and carvedilol best supported by evidence) Side effects • hypotension • bradycardia • peripheral vasoconstriction • impotence • bronchospasm Role of vasodilator therapy • preload (venodilators - nitrates) • afterload (arterial dilators prazosin) • large trials show good benefit but lots of side effects Side effects • hypotension • headache • tachycardia • SLE (hydralazine) Role of Digoxin • used in initial trials • myocardial contractility • lost favour because of toxicity • renally cleared dependent on age, weight & RF Side effects • anorexia • N,V,D • abdominal pain • visual disturbances • drowsiness • arrythmias • heart block Role of spironolactone • improves mortality (RALES) • added into conventional therapy • attenuates aldosterone effect • only small doses required Side effects • hyperkalaemia • gi disturbances • impotence • gynocomastia • rash Adjunct Therapy • Digoxin in SR – – – DIG trial : no mortality benefit but reduction in hospitalisations and improved symptoms useful in symptomatic patients where other drug therapy is optimised should not be withdrawn from pts with HF • Anticoagulation – – if prolonged bed rest : prophylactic heparin if LV dilatation / thrombus : chronic warfarin therapy Mortality remains high • ACEi Risk reduction 35% (mortality and hospitalizations) • Blockers Risk reduction 38% (mortality and hospitalizations) • Oral nitrates and hydralazine Benefit vs. placebo; inferior to enalapril (mortality) However: 4-year mortality remains ~40% Davies Daviesetetal.al.BMJ BMJ2000;320:428-431 2000;320:428-431 Gibbs Gibbsetetal.al.BMJ BMJ2000;320:495-498 2000;320:495-498 Role of other treatments • ?? Ca++ channel antagonists - -ve ionotropic, amlodipine appears safe • ?? other antiarrythmics • dobutamine - increases CO, but palliative • Levosimendan- severe CHF • naturetic peptide inhibitors / recombinant naturetic peptides- omapatrilat / neseritide • Biventricular pacing - severe CHF high cost • transplantation - 85% survival @ 5yrs Congestive cardiac failure Pharmaceutical Care Plan Need for Drug : Selection of Specific Drug: Selection of Regimen: Provision of Drug: Administration of Drug: Monitor Effectiveness: Counsel / Educate: Evaluate Effectiveness: Diagnosis of CHF Symptom control - diuretics Decrease mortality; ACE, B-blockers Co-modibdity: anticoagulation Patient factors Loading doses, maintenance dose Drug factors Timely, accurate Timing, food Symptoms, pulse,cholesterol, side effects Expected effects, side effects Risks vs benefits Beneficial effects > detrimental effects??