Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
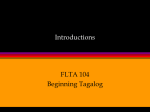
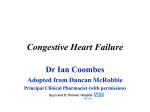
1185 Cardiac Myocyte Necrosis Induced by Angiotensin II Lip-Bun Tan, Jorge E. Jalil, Ruth Pick, Joseph S. Janicki, and Karl T. Weber Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Although the role of angiotensin II (Ang II) in the pathogenesis and progression of the failing heart is uncertain, previous reports have suggested that myocyte injury may be a component in this process. In this study, we investigated this possibility in more detail. Cardiotoxic effects of nonacutely hypertensive doses of Ang II were examined in 90 rats, including those receiving an angiotensin infusion (200 ng/min i.p.) and those with renovascular hypertension, where endogenous stimulation of Ang II occurred. Myocyte injury and wound healing resulting from these treatments were evaluated by 1) immunofluorescence after in vivo monoclonal antibody labeling of myosin to detect abnormal sarcolemmal permeability, 2) [3H] thymidine incorporation into DNA, to detect fibroblast proliferation, and 3) light microscopic evidence of myocytolysis and subsequent scar formation. We found that exogenous Ang II produced multifocal antimyosin labeling of cardiac myocytes and myocytolysis, which were maximal on days 1-2 of the infusion. Subsequently, DNA synthesis rates were increased, with fibroblast proliferation reaching peak levels on day 2 (Ang H-treated rats, 90.0±t18.6 cpm/,ug DNA; control rats, 11.4±2.3 cpm/,ug DNA; p<0.05); microscopic scarring was found on day 14 and represented 0.12±0.02% of the myocardium. Concurrent treatment with both propranolol (30 mg/kg/day s.c.) and phenoxybenzamine (5 mg/kg/day i.m.) did not attenuate Ang II-induced antimyosin labeling. Increased endogenous Ang II, resulting from renal ischemia after abdominal aortic constriction, produced both antimyosin labeling and increased rates of DNA synthesis like that observed with Ang H infusion. Both myocyte injury and fibroplasia were prevented with captopril (65 mg/day p.o.), but this protective effect was not seen with reserpine pretreatment. Infrarenal aortic banding without renal ischemia, on the other hand, produced hypertension without necrosis. We conclude that pathophysiological levels of endogenous as well as low-dose exogenous Ang II were associated with altered sarcolemmal permeability and myocytolysis with subsequent fibroblast proliferation and scar formation. Myocyte injury was unrelated to the hypertensive or enhanced adrenergic effects of Ang II or to hypertension per se. Captopril was effective in preventing myocyte injury in renovascular hypertension. The mechanism(s) responsible for Ang HI-induced necrosis will require further study. (Circulation Research 1991;69:1185-1195) T he neuroendocrine system is widely recognized to play a dominant role in the pathophysiology of congestive heart failure.1-3 Both the adrenergic and renin-angiotensin systems are involved. The commonly acknowledged role of From the Cardiovascular Institute (R.P.), Michael Reese Hospital and Medical Center, and The University of Chicago, Pritzker School of Medicine, Chicago, Ill., the Cardiology Department (L.-B.T.), Killingbeck Hospital, Leeds, UK, the Dept. de Enfermedades Cardiovasculares (J.E.J.), Catholic University of Chile, Santiago, Chile, and the Division of Cardiology (J.S.J., K.T.W.), University of Missouri, Columbia, Mo. Supported in part by National Heart, Lung, and Blood Institute grant R01-HL-31701. L.-B.T. was a recipient of the Travelling Fellowship from the Medical Research Council, UK. Address for reprints: Dr. Karl T. Weber, Division of Cardiology (MA432), University of Missouri, One Hospital Drive, Columbia, MO 65212. Received November 1, 1988; accepted June 7, 1991. these systems in heart failure is in triggering mechanisms that compensate for the reduction in systemic blood flow and perfusion pressure.4 Serum levels of norepinephrine5-7 and angiotensin II (Ang 11)8.9 are each elevated in heart failure at rest and rise even further with physical activity.'0"11 Both neurohumoral agents are also known to raise myocardial protein synthesis and cause myocyte hypertrophy.12-16 Less well known are the roles played by the adrenergic and renin-angiotensin systems in the pathogenesis and progression of the failing heart itself. Pharmacological doses17-21 or pathophysiolog- ical levels22'23 of catecholamines are widely known to produce cardiac myocyte necrosis, although the mechanism of cell death is still unclear.24 Like catecholamines, Ang II infused intravenously in doses that induce acute systemic hypertension has been 1186 Circulation Research Vol 69, No 5 November 1991 Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 shown to cause cardiac myocyte necrosis.25,26 However, it is unknown whether smaller exogenous doses of Ang II that do not induce acute hypertension or elevated endogenous levels of Ang II have a similar toxic effect on the myocardium. The issue of whether Ang II mediates cardiac myocyte necrosis is especially relevant in view of the fact that this condition may be eminently treatable by angiotensin converting enzyme inhibitors. It was our aim, therefore, to determine whether exogenous levels of Ang II, which did not precipitate acute hypertension, were related to the appearance of myocyte necrosis. We sought to further determine whether increased endogenous levels of Ang II, developing in response to renal ischemia, might likewise induce necrosis (vis-a-vis nonrenovascular hypertension). Myocyte injury was assessed directly by in vivo labeling with monoclonal antibodies specific to cardiac myosin,27 a specific and sensitive means of detecting abnormal sarcolemmal permeability in individual myocytes,2128 and standard light microscopic examination of fixed tissue. The woundhealing response, specifically fibroblast proliferation and subsequent replacement fibrosis, was also examined to indirectly confirm the presence and extent of myocyte necrosis. We found that abnormal sarcolemmal permeability and myocytolysis occurred with pathophysiological levels of Ang II and were followed by fibroplasia and scarring. Unlike pretreatment with pharmacological agents that would alternate the catecholamine response to Ang II, captopril prevented both myocyte necrosis and wound healing in renovascular hypertension, whereas myocyte necrosis and wound healing were not observed with infrarenal aorta banding. Materials and Methods Animal Population Experiments were performed on 90 male SpragueDawley rats (190-300 g) maintained on a diet of standard chow (Purina No. 5001, Ralston Purina Co., St. Louis, Mo.) containing 174 meq/kg sodium and 282 meq/kg potassium. The rats were allowed to acclimatize to the housing, with free access to food and tap water for 7 days before entry into the study. Ang II Infusion Thirty-one rats were anesthetized with 35-50 mg/kg i.p. methohexital sodium. Each then underwent an intraperitoneal implantation of an Alzet osmotic minipump (model 2002, Alza Corp., Palo Alto, Calif.) containing Ang II (CIBA-GEIGY, West Caldwell, N.J.) dissolved in 0.O1N acetic acid. The concentration of Ang II was adjusted so that 200 ng/min was delivered at the pump rate of 0.5 ,ul/hr. This dose was selected on the basis of preliminary studies that indicated that it did not produce an immediate elevation in arterial pressure in contrast to the acute hypertensive effects seen with the intra- venous infusion of the same dose. Rats received Ang II for 1-14 days before they were killed. A separate group of rats (n=6), which were untreated or which received an intraperitoneal implant of a minipump containing only the vehicle (0.O1N acetic acid), served as the controls. A third set of rats (n=7) received injections of propranolol (10 mg/kg s.c. three times daily) and phenoxybenzamine (5 mg/kg i.m. once daily) before and during intraperitoneal Ang II infusion. In preliminary experiments, this dose of propranolol maximally suppressed both the hypotensive and chronotropic responses to 1 mg/kg s.c. isoproterenol. It also prevented myocyte necrosis and myocardial hypertrophy induced by this dose of isoproterenol.21 The dose of phenoxybenzamine (t112=24 hours) was in excess of the 1 mg/kg required to maximally reduce the pressure response to 400 ng norepinephrine.29 To minimize weight loss, potassium supplements (0.3% in drinking water) were given after the operation to rats receiving Ang ll.30 Systolic blood pressures, using standard tail-cuff manometry,31 and body weights were measured at 1-2-day intervals. Control rats and those receiving propranolol and phenoxybenzamine were killed 1 and 2 days after insertion of the pumps. Animals were killed with methohexital (35-50 mg/kg i.p.), the thorax was opened, and the heart was quickly excised and placed in ice-cold saline. The great vessels and the atria were carefully trimmed away, and the ventricles were divided into right and left (plus septum) ventricles and weighed. Abdominal Aorta Banding With and Without Renal Ischemia To stimulate increased endogenous production of Ang II, we used a model of renovascular hypertension. Since unilateral renal ischemia in a two-kidney animal is accompanied by systemic hypertension, any observation regarding cell necrosis might be interpreted as secondary to either increased circulating Ang II, hypertension, or both. In an attempt to distinguish these factors, five groups of rats were used. These groups were constructed in the following manner after laparotomy following anesthesia with 35-50 mg/kg i.p. methohexital: In the first group (n=20), abdominal aorta constriction to a diameter of 0.8 mm together with constriction of the right renal artery was performed. This model of renovascular hypertension has been used widely in our laboratory and is known to lead to progressive atrophy of the right kidney and hypertrophy of the contralateral nonischemic kidney.32 A second group (n=5) was similarly operated, except in this group the banding procedure did not involve the renal arteries, and neither kidney appeared ischemic. In a third group (n = 10) of rats, the abdominal aorta and right renal artery were constricted as above, and endogenous catecholamine stores were depleted with a course of reserpine33 before inducing renovascular hypertension. The pretreatment protocol consisted Tan et al Ang II Cardiotoxicity of reserpine (2 mg/kg i.p. on day 1 and 1 mg/kg i.p. on day 2); aortic constriction with right renal stenosis was performed on day 3; and 0.2 mg/kg/day reserpine was given on postoperative days. A fourth group (n=8) with abdominal aorta and right renal artery constriction was pretreated for 2 days with captopril, an angiotensin converting enzyme inhibitor, in the drinking water (2 g/l), and this was continued after the operation. The captopril dosage was equivalent to 65 mg/day based on the mean consumption of 32 ml water/day. A fifth group of rats (n =5), which was surgically treated as described above except the ligature was not tightened, served as a set of sham- Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 operated controls. All rats were killed 1-7 days after abdominal aorta constriction. At this time, the rats were anesthetized with methohexital (35-50 mg/kg i.p.) and artificially ventilated via tracheostomy. A carotid artery was cannulated, and arterial pressure was measured. To approximate the pressure of conscious animals, the reading was taken when arterial pressure was stable for a level of anesthesia that was light but sufficient to prevent spontaneous physical motion by the rat. The rat was given further anesthesia before thoracotomy was performed. After thoracotomy, the heart was rapidly excised and placed in ice-cold saline. The great vessels and the atria were removed, and the ventricles were divided and weighed. Determination of Myocyte Injury Evaluation of myocyte injury resulting from Ang II administration was accomplished by two techniques. The first involved in vivo labeling of myocytes with abnormal sarcolemmal permeability using monoclonal anticardiac myosin.21,28 Each rat received 1 mg immunoglobulin G fraction of monoclonal antibody CCM-52 intraperitoneally 24 hours before death. The antibody used in this study, CCM-52, has been shown to be specific for cardiac myosin.27 Antibody administered intraperitoneally appears in the serum in less than an hour, reaches a maximal serum -titer by 3 hours, and remains well above a 1:100 dilution titer necessary for immunofluorescent staining for more than a week (authors' unpublished data). After removal of the heart, 2-mm-thick transverse sections of the left ventricle were quick-frozen in isopentane cooled to the freezing point (- 160°C) in liquid nitrogen. After cryostat sectioning of the heart, the sections were stained with fluorescein isothiocyanate-conjugated rabbit anti-mouse immunoglobulin G (Cappel Laboratories, Cochranville, Pa.) to localize myocyte binding antimyosin monoclonal antibody. Immunofluorescent staining was evaluated with a microscope (Carl Zeiss, Inc., Thornwood, N.Y.) equipped with epifluorescent optics optimized for fluorescein isothiocyanate fluorescence. The second technique used to assess myocyte injury was based on light microscopic examination of formalin-fixed left ventricular tissue sections stained with hematoxylin and eosin. Specifically, we examined a coronal section of the ventricle (free wall and 1187 septum) for evidence of myocytolysis, based on a disruption of the internal cellular architecture. The entire left ventricular myocardium was scanned in a clockwise fashion beginning at the endocardial surface of the septum. Whenever an area of myocytolysis was found, its location and approximate size with respect to the starting point were noted on a standardized diagram of a left ventricular cross section. Determination of Wound Healing DNA synthesis in heart tissue of each experimental group was analyzed by estimation of total incorporation of [3H]thymidine into DNA. [methyl3H]Thymidine (TRK.686, specific activity >50 Ci/ mmol, Amersham, Arlington Heights, Ill.) was administered by intraperitoneal injection (1 ,Ci/g body wt) 4 hours before death. Thymidine incorporation into DNA was determined as described by Benjamin et al.21 Immediately after the heart was excised and weighed, the right and left ventricles were finely minced with scissors and homogenized with a Polytron (Brinkmann Instruments, Inc., Westbury, N.Y.) in 2 ml ice-cold phosphate-buffered saline. Two milliliters of cold 10% trichloroacetic acid was added to the homogenate to precipitate DNA and proteins. The tissue homogenates were centrifuged and washed three times with 3 ml cold 5% trichloroacetic acid and then with a final rinse of 3 ml of 2% sodium acetate in 90% ethanol to remove unincorporated [3H]thymidine. After centrifugation, the supernatant was discarded, and the precipitates were resuspended in 2 ml of 5% trichloroacetic acid. DNA was extracted by heating the samples at 90°C for 30 minutes. After centrifugation, aliquots of the supernatant were taken for determination of tritium radioactivity by scintillation counting and of DNA content by the method of Burton.34 DNA standards were prepared from calf thymus DNA, and the concentrations of the standard were determined by its absorbance at 260 nm. Stimulation of DNA synthesis was determined from the specific radioactivity (cpm/,g DNA) in each tissue sample. Subsequent scarring of the myocardium was examined using a collagen-specific stain, sirius red F3BA. Here coronal sections of the left ventricle were examined at day 14 of the Ang II infusion and after 2 weeks of renovascular or nonrenovascular hypertension. Similar analysis of myocardium was performed in control rats. The slide was placed in a projecting microscope, and the image was projected onto a digitizing pad. The entire left ventricular cross section was scanned (magnification, x40) with the investigator (R.P.) blinded as to the source of the tissue. Whenever an area of replacement fibrosis, as represented by the presence of confluent fibrillar collagen in regions formerly occupied by myocytes, was found, its contour was traced, and the area within the contour was calculated. The entire area of muscle was also obtained, and the collagen volume fraction of replacement fibrosis was calculated as the 1188 Circulation Research Vol 69, No 5 November 1991 sum of all sampled areas containing lesions divided by the sum of all areas with and without lesions. The density of fibrotic areas was expressed as number of foci per square millimeter. Statistical Analysis The grouped results are expressed as mean±SEM and were compared using the Kruskal-Wallis analysis of variance (BMDP, Los Angeles). When a significant intergroup difference was found, then pairwise comparisons were performed by calculating confidence intervals for the rank differences. Statistical significance was set at p<0.05. Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Results Cardiac Myocyte Necrosis After Ang II Infusion Antimyosin labeling of cardiac myocytes was observed within 24 hours of intraperitoneal infusion of Ang II. A scattered multifocal distribution of labeled myocytes was found throughout the myocardium (see Figure 1), with some tendency toward clustering of antibody-labeled myocytes around the perivascular regions of intramyocardial arteries and arterioles. In contrast to antibody labeling after isoproterenol treatment,2' labeled myocytes resulting from Ang II infusion were not preferentially distributed in the subendocardial region. The number of labeled myocytes peaked between days 1 and 2 and declined thereafter. At no time was there any myocyte labeling detected in rats treated with minipumps containing the O.O1N acetic acid vehicle. Myocytolysis was evident on light microscopic examination on day 2 of the Ang II infusion; it was not observed in control rats. Myocyte necrosis was patchy and distributed throughout the myocardium without a discernible pattern of distribution. Occasionally, large numbers of myocytes were involved (see Figure 2, top panel). In most cases, however, myocytolysis was confined to small numbers of cells and accompanied by fibroblast proliferation (see Figure 2, bottom panel). Effect of Adrenergic Hormone Antagonists To rule out the possibility that myocyte necrosis in the heart occurred secondary to enhanced adrenergic hormone release facilitated by Ang II, we used adrenergic hormone antagonists to block this effect. The prior and concurrent treatment with a- and ,B-adrenergic inhibitors did not attenuate the necrotic effects of infused Ang II. The pattern and extent of myocyte necrosis with Ang II and the combination of propranolol and phenoxybenzamine were similar to those seen with Ang II alone. It should be noted that the same level of propranolol applied in a prior study21 completely blocked the necrogenic effects of 1 mg/kg isoproterenol. Thus, Ang II-mediated myocyte necrosis observed in this study did not result from secondary adrenergic hormone activity. Cardiac Myocyte Necrosis After Abdominal Aorta Banding Since cardiac myocyte necrosis was detected after intraperitoneal Ang II infusion, we sought to determine whether Ang II arising from stimulation of the renin-angiotensin system after renal ischemia might generate a similar response. Thus, we examined hearts of rats treated with monoclonal antimyosin at 1-7 days after surgical induction of renovascular hypertension. To evaluate whether the myocardial response resulted from surgical manipulation, aortic constriction, or renin production after renal ischemia, myocyte injury was compared in sham-operated and abdominal aorta-banded rats with and without right renal artery constriction. At the time of the study, rats with banding of the abdominal aorta including constriction of the right renal artery had an ischemic-appearing right kidney; the left kidney appeared well perfused. In rats without renal ischemia, both kidneys appeared well perfused. In rats with renovascular hypertension, antimyosin-labeled necrotic myocytes were found throughout the myocardium. Labeling was most numerous on postoperative day 1, and the pattern and distribution of labeling were similar in appearance to those seen with Ang Il-induced necrosis. In rats without renal ischemia, no myocyte necrosis was detected. Prior depletion of endogenous catecholamine stores with reserpine pretreatment did not attenuate the cardiac myocyte necrosis associated with renal artery constriction. In renovascular hypertension, light microscopic evidence of myocytolysis was seen to involve individual myocytes in a diffuse, random distribution throughout the myocardium. This was not the case in nonrenovascular hypertension, where myocytes appeared intact. Effect of Captopril Further evidence that Ang II was the active factor in generation of myocyte injury was provided by evaluation of the effect of captopril on myocyte necrosis in rats with abdominal aorta constriction. When rats having abdominal aorta constriction with renal ischemia were treated with captopril, antibody-labeled cardiac myocytes were not seen on serial sections. Increased Cardiac DNA Synthesis A direct response to cardiac myocyte injury is cardiac fibroblast proliferation, which may be detected with great sensitivity by the increase in cardiac DNA synthesis rates. Thus, an independent confirmation of myocyte injury is provided by assessment of rates of tritiated thymidine incorporation. We observed that the rate of ['H]thymidine incorporation closely paralleled the appearance of necrotic myocytes in the heart after Ang II infusion. The rate of ['H]thymidine incorporation in the left ventricle increased slightly on the first day of Ang II infusion, reached a peak on day 2, and declined rapidly thereafter (Figure 3). Tan et al Ang II Cardiotoxicity 1189 Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 FIGURE 1. Photomicrographs showing angiotensin II-induced cardiac myocyte necrosis. The necrotic cells were labeled by in vivo administration of monoclonal antimyosin and postmortem staining of tissue sections with fluorescein isothiocyanate-conjugated rabbit anti-mouse immunoglobulin G. Permeable necrotic cells admit the monoclonal antibody and are thus stained with the fluorescein isothiocyanate-conjugated secondary antibody and appear as the bright cells in the photographs. Magnification, x148.75 for top panel and x374 for bottom panel. The time course of stimulation of DNA synthesis in renal ischemia was similar to that seen with Ang II infusion, being maximal on postoperative day 2. The peak rate of DNA synthesis on day 2 was also of the same order of magnitude as that seen with Ang II infusion (Figure 4). In rats with aortic banding without right renal artery constriction, the DNA synthesis rate was not different from that of controls (19.5+±5.5 cpm/gg for banded rats versus 11.4±2.3 cpm/gg for controls). In rats with abdominal aorta 1190 Circulation Research Vol 69, No 5 November 1991 Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 FIGURE 2. Light microscopic evidence of myocytolysis observed on day 2 of angiotensin II infusion together with inflammatory cell and fibroblast infiltration in the region of cell injury. Occasionally, large numbers of myocytes were involved (top panel). In most cases, however, myocytolysis was confined to small numbers of cells and was accompanied by mononuclear cell infiltrates and fibroblast proliferation (bottom panel). Stain, hematoxylin and eosin; magnification, x36 for top and bottom panels and x 90 for insert to bottom panel. Tan et al Ang II Cardiotoxicity Rates of DNA Synthesis during AII Infusion 1191 251 20 t)o N. 8 0. 04 15 l40 w W k- w ¢ 10 LL ii U We 0.4 C) 5 a 1 0 2 4 6 8 DAYS 10 12 14 FIGURE 3. Graph showing the specific radioactivity of [3Hlthymidine incorporation into DNA produced by angiotenDownloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 sin II (AII) infusion for 1-14 days (day O=sham-operated rats). Rats were pulse-labeled for 4 hours with [3H]thymidine on the days indicated. After death by methohexital, DNA was extracted, and the specific radioactivity (cpm/pg DNA) was determined. Elevated specific radioactivities indicate increased cell proliferation. *p<0.05 compared with day 0. constriction and right renal ischemia, which were also treated with captopril, the rate of DNA synthesis was not elevated and was similar to that observed in sham-operated rats (Figure 4). Replacement Fibrosis In picrosirius red-prepared sections, punctate foci of microscopic scarring were evident throughout the left ventricular myocardium. The number of scars per square millimeter found in hearts receiving the Ang II infusion for 14 days was 0.5+±0.1, and the average size of the scars was 2,950±500 gm2. As shown in Figure 5, the majority of scars were <4,500 ,um2; hence, the reparative fibrosis occurred in only 0.12+0.02% of the myocardium and is in keeping with necrosis of myocytes. No scarring was found in control hearts. Effects of Ang II and Abdominal Aorta Constriction on Blood Pressure Intraperitoneal Ang II infusion did not cause a significant rise in arterial pressure during the first 3 o0 625 1500 2600 3300 4500 5300 6800 SCAR SIZE (pm2) FIGURE 5. Bar graph showing frequency distribution of microscopic scars found scattered throughout the myocardium in rats receiving intraperitoneal angiotensin II infusion for 14 days. The number and size of these scars were detected by the picrosirius red technique. days of infusion. Thereafter, a gradual rise in systolic pressure was observed, which reached a peak on the 10th day (Figure 6), when systolic arterial pressure exceeded 200 mm Hg. With surgical constriction of the abdominal aorta, the systolic carotid artery pressure immediately before death was 187+10 mm Hg in rats with right renal artery constriction and 173 + 10 mm Hg in rats without right renal constriction as compared with 138 +3 mm Hg obtained in the sham-operated controls. The rate of increase in blood pressure was not determined after abdominal aorta constriction, since tail-cuff pressures could not be taken after this procedure. Pretreatment with captopril in the abdominal aorta constriction with renal ischemia model prevented the elevation in systolic blood pressure (119±4 mm Hg) as compared with the untreated group (187 mm Hg). Effects of Ang II and Abdominal Aorta Constriction on Myocardial Hypertrophy The combined ventricular weights normalized to body weights were increased by 10-12% during Ang Systolic BP during AII infusion 150- 100 * 200 R 0.. U to 50. 0 M 0. u) 150- U) 0o SHA AAE +RI RI R+C FIGURE 4. Bar graph showing DNA specific radioactivity on day 2 in rats treated with angiotensin II (A II), aortic banding with (+) and without (-) renal ischemia (RI), and renal ischemia with concurrent captopril (RI+C). Values are mean+±SEM. *p<0.05 vs. sham-operated rats (SHAM). 100- . 0 2 4 6 8 DAYS 10 12 14 FIGURE 6. Graph showing mean+±SEM systolic arterial blood pressure (BP) during 14 days of angiotensin II (AII) infusion. *p<0.05 vs. day 0. 1192 Circulation Research Vol 69, No 5 November 1991 II infusion relative to controls, reaching a peak at day 14 on continued infusion. The ventricular weight normalized to body weight increased from 2.98+±0.05 g/kg in controls to 3.41±0.13 g/kg after 2 weeks of sustained Ang II infusion. A similar observation was noted in the rats with abdominal aorta banding, with normalized ventricular weights rising from 2.98± 0.05 g/kg in control rats to 3.76±0.20 g/kg on day 7 after the operation. The ventricular weight/body weight ratios were not increased after renal ischemia in the group treated with captopril (2.63±0.06 g/kg). Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Discussion Association ofAng II With the Genesis of Cardiac Myocyte Necrosis Using in vivo labeling with monoclonal antimyosin, we have shown that both Ang II infusion and endogenous Ang II, arising as a consequence of renal ischemia, are associated with the development of cardiac myocyte necrosis. This necrosis does not appear to be mediated by either adrenergic activation or systemic hypertension, which are both known to result from Ang II. Furthermore, when augmented synthesis of Ang II by concurrent captopril treatment in the renovascular hypertension model was prevented, myocyte injury and wound healing were not seen. The development of cardiac myocyte injury in the setting of renal ischemia is consistent with earlier reports.35-37 Infusion of ischemic renal extracts was shown to produce myocyte injury; however, this injury was absent with removal of the ischemic kidney.37 Whether this effect could be attributed to endogenous angiotensin has not been established.38 Our experiments provide new evidence for the role of endogenous Ang IL in the genesis of cardiac myocyte necrosis in renovascular hypertension and in congestive heart failure, where endogenous circulating Ang II achieves levels similar to those seen in this study (see below). Stimulation of DNA synthesis and scar tissue formation serve as an independent confirmation of myocyte necrosis and are indicative of the woundhealing process that involves fibroblast proliferation and collagen replacement of cell loss. Both Ang II infusion and renovascular hypertension resulted in enhanced myocardial DNA synthesis and replacement fibrosis. The rate of increase and scarring closely paralleled the pattern of necrosis observed with antimyosin labeling. The fact that concurrent treatment with captopril (by preventing excess Ang II synthesis) abolished myocyte necrosis and the subsequent increase in DNA synthesis rates provides further evidence that elevated endogenous Ang II was responsible for abnormal sarcolemmal permeability and myocytolysis. The cardioprotective effect of captopril is of clinical importance, in that the progression of cardiac dysfunction secondary to myocyte loss induced by elevation of endogenous Ang II levels can be effectively treated by angiotensin converting enzyme inhibition. Ang II-Mediated Necrosis Secondary to Hypertension Previous studies have shown that large doses of Ang II can cause focal myocardial injury.26,39 It is currently believed that this injury occurs in close conjunction with the hypertension induced by Ang 11.25 Using a model of renovascular hypertension, Bhan et a135 observed foci of myocardial damage in the subendocardium of the left ventricle; these foci were thought to be consistent with ischemic or anoxic or reflow injury. They also observed vascular lesions in epicardial and intramyocardial arteries that were related to the severity of hypertension in the case of epicardial vessels and to the vasoconstrictive action of Ang II in the case of intramural vessels. Bhan et al40 subsequently extended their study and showed that when the hypertensive effects of 1,700 ng/kg/min i.v. Ang II were counteracted by concurrent phentolamine treatment, Ang II produced vascular injury confined to intramyocardial coronary arteries, with minimal evidence of myocyte injury. This suggests that irreversible myocardial injury is dependent on the hypertensive and vasoconstrictive effects of Ang II. Our study is the first to demonstrate that Ang II given in a manner that does not induce acute hypertension is involved in the generation of cardiac myocyte necrosis, suggesting that the mechanisms producing necrosis are independent of the hypertensive effects of Ang II. In fact, as arterial pressure gradually rose with the sustained infusion of Ang II, no new injury could be detected in our study. Additional corroborative evidence supporting the dissociation between necrosis and hypertension is provided by evidence that abdominal aorta constriction applied in a manner that did not produce renal ischemia results in hypertension but not in myocyte necrosis. It is not clear why myocyte necrosis in the absence of hypertension was detected in our study, whereas it appears not to have been detected in the study of Bhan et al.40 Plasma Ang II Levels The dose range of Ang II infusion used in our experiment (0.6-1.0 ,ug/kg/min) was only marginally smaller than the ones used in other studies (0.9-1.8 j.tg/kg/min).26,39 However, we used an intraperitoneal rather than intravenous route of administration. Plasma Ang II levels of 70.6±6.4 pg/ml were determined after 24 hours of intraperitoneal infusion. This was similar to the levels of plasma Ang II seen at 24 hours in the rats with abdominal aorta banding and renal ischemia (56.7±21.9 pg/ml). These levels are well within the pathophysiological range reported in cases of essential hypertension (147-189 pg/ml),41 renal hypertension (154+±93 pg/mI),42 and severe heart failure (28-155 pg/ml).43,44 Our normal control rats had levels of 9.5±3.5 pg/ml. Intravenous infusion of Ang II at 200 ng/min produced plasma levels in excess of 400 pg/ml and an Tan et al Ang II Cardiotoxicity acute hypertensive response, whereas intraperitoneal infusion at the same dose produced lower plasma levels and no acute hypertensive response. The differences may be due to the inactivation of the intraperitoneal Ang II by angiotensinase in the liver, lungs, and kidneys.43 Whether Ang II metabolites are responsible for the observed lesions cannot as yet be ascertained and would form an essential part of future studies to elucidate the mechanism(s) of Ang Il-induced cardiomyocyte necrosis. Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Relation Between Necrotic and Vasculotoxic Effects of Ang II Epicardial coronary artery constriction has been observed with intracoronary infusion of Ang II.45 Whether the mechanism of necrosis involved vasculotoxic or vasoconstrictive effects of Ang II on intramyocardial coronary arteries has not been resolved. Giacomelli et a125 showed that foci of myocardial injury produced by intravenous infusion of 1,700 ng/kg/min Ang II were observed in areas that have no consistent topographic relation to these intramural arteries. They speculated that the myocardial damage was secondary to ischemic or anoxic injury, with or without reflow damage. Bhan et al35,40 have suggested a similar relation between the vasculotoxic and myocyte necrotic effects of Ang II. Although these studies suggest a vasculotoxic effect, they do not conclusively demonstrate that the myotoxic effect of Ang II is secondary to vascular effects. Ideally, to demonstrate that the myocardial lesions are secondary to coronary vascular lesions, one needs to show that myocyte necrosis resides in regions distal to the vascular lesions. The correlative method used in the study of Bhan et al,40 who showed increased myocardial lesions in hearts with increased vascular lesions, cannot lead to any firm conclusion about the spatial relation of the lesions. Permeability of systemic and intramural arteries is abnormally increased by Ang 11.25,46-48 Thus, myocytes adjacent to arterioles may be subject to a cascade of events, including the release of vasoactive amines,49 that leads to sarcolemmal disruption and ultimately cell death. Further studies are required to elucidate the relation between augmented vessel permeability, release of vasoactive amines, and cell death due to low-dose Ang II infusion. Adrenergic Activation as a Mechanism Several lines of evidence suggest that angiotensininduced necrosis is not mediated by sympathetic activation or catecholamine release. In contrast to the pattern of necrosis produced after intraperitoneal infusion of 200 ng/min Ang II, isoproterenol characteristically produces subendomyocardial necrosis.1821 In addition, doses of propranolol and phenoxybenzamine that were effective in inhibiting the hemodynamic response to high levels of circulating catecholamines and that totally blocked isoproterenol-induced myocardial injury did not block angiotensin-induced myocyte necrosis. Further evidence that Ang TI-mediated cardio- 1193 myocyte necrosis was not due to secondary catecholamine release is provided by the observation that the same extent of necrosis occurred after reserpine depletion of catecholamine stores before renal artery constriction, as occurred in the absence of reserpine treatment. Thus, Ang II appeared to produce cardiac myocyte necrosis independent of the cardiotoxicity that might result from sympathetic activation or facilitated release of catecholamines. Role of Ang II Receptors Whether the cardiotoxic effects of Ang II are mediated through myocardial receptors is uncertain. It is notable that Ang II receptors have not been demonstrated at the same level in the adult rat heart as have been found in other species (e.g., rabbit, guinea pig, and bovine myocardium; T.B. Rodgers, personal communication). The explanation is unclear, especially in view of the fact that the same techniques have demonstrated a high density of angiotensin receptors in neonatal rat cardiac myocytes.50 Therefore, we cannot suggest that cardiac myocyte necrosis resulting from Ang II infusion or abdominal aorta constriction is mediated by Ang II binding to cardiac myocyte receptors. Robertson and Khairallah51 reported binding of Ang II in nuclei of rat cardiac muscle. Whether nuclear or other hitherto unknown types of binding play a role in mediating Ang II effects in adult rat myocardium is unclear. That the adult rat heart is responsive to Ang II was demonstrated by Xiang et al,52 who showed that Ang II added to the perfusate in Langendorff preparations increased contractile force in adult rat hearts. Conclusion We have demonstrated that Ang II arising either from endogenous or exogenous sources is associated with the appearance of abnormal sarcolemmal permeability, myocytolysis, fibroblast proliferation, and subsequent replacement fibrosis. It is not clear whether Ang II acts directly through myocyte receptors to produce this effect nor whether a metabolite of Ang II might be the active factor in this process. Our data do appear to exclude secondary adrenergic stimulation and arterial hypertension as being responsible for this effect. The mechanism by which Ang IL leads to myocyte necrosis remains to be determined. Acknowledgments We thank Smith Kline & French for the supply of phenoxybenzamine and Dr. Ron White of E.R. Squibb & Sons for conducting the plasma Ang II assays. References 1. Laragh JH: Hormones in the pathogenesis of congestive heart failure: Vasopressin, aldosterone, angiotensin II. Circulation 1962;25:1015-1023 2. Harris P: Evolution and the cardiac patient. Cardiovasc Res 1983;17:437-445 3. Francis GS: Neurohumoral mechanisms involved in congestive heart failure. Am I Cardiol 1985;55:15A-21A 1194 Circulation Research Vol 69, No 5 November 1991 4. Harris P: Congestive cardiac failure: Central role of the arterial blood pressure. Br Heart J 1987;58:190-203 5. Cohn JN, Levine TB, Olivary MT, Garberg V, Lura D, Francis GS, Simon AB, Rector T: Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med 1984;311:819-823 6. Hasking GJ, Esler MD, Jennings GL, Burton D, Johns JA, Korner PI: Norepinephrine spillover to plasma in patients with congestive heart failure: Evidence of increased overall and cardiorenal sympathetic nervous activity. Circulation 1986; 73:615-621 7. Leimbach WN, Wallin G, Victor RG, Aylward PE, Sundlof G, Mark AL: Direct evidence from intraneural recordings for increased central sympathetic outflow in patients with heart Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 failure. Circulation 1986;73:913-919 8. Cleland JGF, Dargie HJ, Hodsman GP, Ball SG, Robertson JIS, Morton JJ, East BW, Robertson I, Murray GD, Gillen G: Captopril in heart failure: A double blind controlled trial. Br Heart J 1984;52:530-535 9. Cleland JGF, Dargie HJ, Robertson I, Robertson JIS, East BW: Total body electrolyte composition in patients with heart failure: A comparison with normal subjects and patients with untreated hypertension. Br Heart J 1987;58:230-238 10. Chidsey CA, Harrison DC, Braunwald E: Augmentation of the plasma norepinephrine response to exercise in patients with congestive heart failure. N Engl J Med 1962;267:650-654 11. Francis GS: Hemodynamic and neurohumoral responses to dynamic exercise: Normal subjects versus patients with heart disease. Circulation 1987;76(suppl VI):VI-11-VI-17 12. Re RN: Cellular mechanisms of growth in cardiovascular tissue. Am J Cardiol 1987;60:1041-1091 13. Upsher ME, Khairallah PA: ,B-Adrenergic receptors in rat myocardium during the development and reversal of hypertrophy and following chronic infusions of angiotensin II and epinephrine. Arch Int Pharmacodyn 1985;274:65-79 14. Khairallah PA, Kanabus J: Angiotensin and myocardial protein synthesis, in Tarazi RC, Dunbar JB (eds): Perspectives in Cardiovascular Research. New York, Raven Press, Publishers, 1983, vol 8, pp 337-347 15. Chappel CI, Rona G, Balazs T, Gaudry R: Comparison of cardiotoxic actions of certain sympathomimetic amines. Can J Biochem Physiol 1959;37:35-42 16. Rosenblum I, Wohl A, Stein AA: Studies of cardiac necrosis: I. Production of cardiac lesions with sympathomimetic amines. Toxicol Appl Pharmacol 1965;7:1-8 17. Todd GL, Cullan GE, Cullan GM: Isoproterenol-induced myocardial necrosis and membrane permeability alterations in the isolated perfused rabbit heart. Exp Mol Pathol 1980;33: 43-54 18. Collins P, Billings CG, Barer GR, Daly JJ, Jolly A: Quantitation of isoprenaline-induced changes in the ventricular myocardium. Cardiovasc Res 1975;9:797-806 19. Reichenbach DD, Benditt EP: Catecholamines and cardiomyopathy: The pathogenesis and potential importance of myofibrillar degeneration. Hum Pathol 1970;I:125-150 20. Bloom S, Cancilla PA: Myocytolysis and mitochodrial calcification in rat myocardium after low doses of isoproterenol. Am JPathol 1969;54:373-391 21. Benjamin IJ, Jalil JE, Tan LB, Cho K, Weber KT, Clark WA: Isoproterenol-induced myocardial fibrosis in relation to myocyte necrosis. Circ Res 1989;65:657-670 22. Alpert LI, Pai SH, Zak FG, Wertheimer S: Cardiomyopathy associated with pheochromocytoma. Arch Pathol 1972;93: 544-548 23. Cho T, Tanimura A, Saito Y: Catecholamine-induced cardiopathy accompanied with pheochromocytoma. Acta Pathol Jpn 1987;37:123-132 24. Rona G: Catecholamine cardiotoxicity. J Mol Cell Cardiol 1985;17:291-306 25. Giacomelli F, Anversa P, Wiener J: Effect of angiotensininduced hypertension on rat coronary arteries and myocardium. Am J Pathol 1976;84:111-138 26. Gavras H, Brown JJ, Lever AF, Macadam RF, Robertson JIS: Acute renal failure, tubular necrosis, and myocardial infarc- 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. tion induced in the rabbit by intravenous angiotensin II. Lancet 1971;2:19-22 Clark WA, Chizzonite RA, Everett AW, Rabinowitz M, Zak R: Species correlations between cardiac isomyosins: A comparison of electrophoretic and immunological properties. J Biol Chem 1982;257:5449-5454 Nolan AC, Clark WA, Karwoski T, Zak R: Patterns of cellular injury in myocardial ischemia determined by monoclonal antimyosin. Proc Natl Acad Sci U S A 1983;80:6046-6050 Paller MS, Linas SL: Role of All, a-adrenergic system, and arginine vasopressin on arterial pressure in rat. Am J Physiol 1984;246:H25-H30 Garwitz ET, Jones AW: Aldosterone infusion into the rat and dose-dependent changes in blood pressure and arterial ionic transport. Hypertension 1982;4:374-381 Lovenberg W: Techniques for the measurement of blood pressure. Hypertension 1987;9(suppl I):I-5-I-6 Weber KT, Janicki JS: Angiotensin and the remodeling of the myocardium. Br J Clin Pharmacol 1989;28:141S-150S Antonaccio MJ, Smith CB: Effects of chronic pretreatment with small doses of reserpine upon adrenergic nerve function. J Pharmacol Exp Ther 1974;188:654-667 Burton K: A study of the conditions and mechanism of the diphenylamine reaction for colorimetric estimation of deoxyribonucleic acid. Biochem J 1956;62:315-323 Bhan RD, Giacomelli F, Wiener J: Ultrastructure of coronary arteries and myocardium in experimental hypertension. Exp Mol Pathol 1978;29:66-81 Winternitz MC, Mylon E, Waters LL, Katzenstein R: Studies on the relation of the kidney to cardiovascular disease. Yale J Biol Med 1940;12:623-679 Muirhead EE: Renal tissue and extracts vs cardiovascular injury. Arch Pathol 1963;76:613-619 Fernandez LA, Downing E: Cardiomyopathy produced in rats with acute renal hypertension. J Lab Clin Med 1980;95: 159-167 Gavras H, Kremer D, Brown JJ, Gray B, Lever AF, MacAdam RF, Medina A, Morton JJ, Robertson JIS: Angiotensin- and norepinephrine-induced myocardial lesions: Experimental and clinical studies in rabbits and man. Am Heart J 1975;89: 321-332 Bhan RD, Giacomelli F, Wiener J: Adrenergic blockade in angiotensin-induced hypertension: Effect on rat coronary arteries and myocardium. Am J Pathol 1982;108:60-71 Dusterdieck G, McElwee G: Estimation of angiotensin II concentration in human plasma by radioimmunoassay: Some applications to physiological and clinical states. Eur J Clin Invest 1971;2:32-38 Catt EJ, Cain MD, Coghlan JP, Zimmet PZ, Cran R, Best JB: Metabolism and blood levels of angiotensin II in normal subjects, renal disease and essential hypertension. Circ Res 1970;26/27(suppl II):II-177-II-193 Staroukine M, Devriendt J, Decoodt P, Verniory A: Relationship between plasma epinephrine, norepinephrine, dopamine and angiotensin II concentrations, renin activity, hemodynamic state and prognosis in acute heart failure. Acta Cardiol 1984;39:131-138 Kuroda T, Shida H: Angiotensin II-induced myocardial damage with a special reference to low cardiac output syndrome. Jpn Heart J 1983;24:235-243 Cohen MV, Kirk ES: Differential response of large and small arteries to nitroglycerin and angiotensin. Circ Res 1973;33: 445-453 Robertson AL, Khairallah PA: Effects of angiotensin II and some analogues on vascular permeability in the rabbit. Circ Res 1972;31:923-931 Giese J: Renin, angiotensin and hypertensive vascular damage: A review. Am J Med 1973;55:315-332 Wiener J, Giacomelli F: The cellular pathology of experimental hypertension: VII. Structure and permeability of the mesenteric vasculature in angiotensin-induced hypertension. Am J Cardiol 1973;72:221-240 Tan et al Ang II Cardiotoxicity 49. Fantone JC, Schier D, Weingarten B: Inhibition of vascular permeability changes in rats by captopril. J Clin Invest 1982; 69:1207-1211 50. Rogers TB, Gaa ST, Allen IS: Identification and characterization of functional AII receptors on cultured heart myocytes. J Pharmacol Exp Ther 1986;236:438-444 51. Robertson AL, Khairallah PA: Angiotensin II: Rapid localization in nuclei of smooth and cardiac muscle. Science 1971; 172:1138-1139 1195 52. Xiang J, Linz W, Becker H, Ganten D, Lang RE, Scholkens B, Unger T: Effects of converting enzyme inhibitors ramipril and enalapril on peptide action and sympathetic neurotransmission in the isolated heart. Eur J Pharmacol 1985;113:215-223 KEY WORDS * monoclonal antimyosin * renovascular hypertension * captopril * myocardial fibrosis Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Cardiac myocyte necrosis induced by angiotensin II. L B Tan, J E Jalil, R Pick, J S Janicki and K T Weber Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Circ Res. 1991;69:1185-1195 doi: 10.1161/01.RES.69.5.1185 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1991 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/69/5/1185 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/