Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
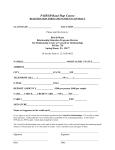
PatientMedicalHistory/SubjectiveSummary PatientName:______________________________________________DateofBirth:____________________________ Occupation:________________________________________________________________________________________ DailyActivitiesatWork:______________________________________________________________________________ DailyActivitiesatHome:______________________________________________________________________________ Hobbies:__________________________________________________________________________________________ Brieflygiveahistoryofyourinjury–Whyareyouhere? __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Pastmedicalhistory:(Pleaselistmedications,ailments,pastinjuries,conditions,accidents,traumas). __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Listprevioussurgeriesanddates:_______________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Doyouhaveanyofthefollowingmedicalconditions?Circleallthatapply: _____RheumatoidArthritis _____Osteoarthritis _____AutoimmuneDisorders_____HighBloodPressure _____LowBloodPressure _____Dizziness _____Shortnessofbreath_____Cancer__________ _____VisualDisturbances _____Asthma _____Pregnancy _____Pacemaker _____Implants_________________________________Siezures _____Diabetes _____Depression_____ThyroidHigh/Low _____WeightLoss/Gain>20lbs _____HistoryofFalls _____CardiacorVascularissues_____________________________________________________ _____Headaches OTHERS:___________________________________________________________________________________________ Haveyouhadanyofthefollowingforthiscondition:______X-Ray,______MRI,______EMG,______ Other:____________________. PatientMedicalHistory/SubjectiveSummary Ifso,areyouawareoftheresultsofthesetests?Explain:___________________________________________________ __________________________________________________________________________________________________ Haveyouhadtreatmentforthisconditionbefore?Yes______No_______ Ifyes,whenandwhatdidyoureceivetreatmentandwhatwastreatment?___________________________________ __________________________________________________________________________________________________ Doyouhaveanyknownallergies?_______Yes ________No Ifyes,pleasedescribe:_______________________________________________________________________________ Doyouexerciseregularly? ________Yes________No Ifyes,whatdoyoudoandhowoften? __________________________________________________________________________________________________ WhatareyourgoalsforPhysicalTherapy?_______________________________________________________________ __________________________________________________________________________________________________ Pleaseindicatetheamountofpainyouareexperiencingwithyourcurrentcondition: 0 1 2 3 4 5 6 7 8 9 Pleaseshadeinareasofpainonthediagrambelow: Key: Numbness:====== Pins/Needles:oooo BurningPain:xxxxxx StabbingPain:////// PatientSignature:_______________________________________________Date:_____/_______/20_________ TherapistSignature:_____________________________________________Date:_____/_______/20_________ 10