Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
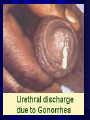
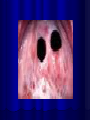
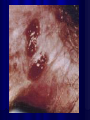
Sexually Transmitted Diseases Presented by Felecia Briggs RN, MS, APN-BC June 4th, 2010 Student Objectives The students will be able to: differentiate between the common signs and symptoms of Chlamydia, Gonorrhea, Herpes, Syphilis, Hepatitis B, and HIV. List three alternatives to having unprotected sex Understand the possible consequences of not using condoms, if sexually active Understand the importance of being more proactive about their health (i.e., annual checkups, use of condoms, practicing monogamy, avoiding drug and alcohol use during sex, or being abstinent). National Surveillance Rates Sexually transmitted diseases (STDs) remain a major public health challenge in the United States. While tremendous progress has been made in preventing, diagnosing, and treating certain STD’s-the CDC estimates that 19 million new infections occur each year (MMWR, 2005). More than half of the STD cases occur amongst young people between the ages of 15-24. Sexually Transmitted Diseases STD’s fall into three categories, bacterial, viral, or parasitic Bacterial infections can be completely cured Viral infections may clear up in 4-6 weeks, but some may remain for the rest of your life Parasitic Infections- although annoying and uncomfortable, they can usually be cured quite easily Bacterial Infections Chlamydia- an STD caused by intracellular parasitic organism CTrachomatis, which causes 1. Pelvic inflammatory disease 2. Ocular infections 3. Lymphogranuloma venereum- primarily infects the lymphatics 5. Acute urethral syndrome in females 6. Reiters syndrome- a disorder that causes three seemingly unrelated symptoms: arthritis, redness of the eyes, and urinary tract signs. * Up to 85% of women and 25% of men are asymptomatic Chlamydia Defined? Chlamydia is the most commonly transmitted STD, and it’s caused by the bacterium called “Chlamydia Trachomatis”-which can damage a women’s reproductive organs. It’s transmitted during vaginal, anal or oral sex. Also, passed from mother to baby during childbirth. Known as the silent disease, because ¾ of women and ½ infected men have no symptoms. Men may have d/c from their penis or burning w/urination, some may have a burning/itching feeling around the opening of the penis Who does Chlamydia Affect? African American women are disproportionately affected by chlamydia. For instance, rates per 100,000 black females was 1,729.0-seven times (7X) that of White females (237.2) and more than twice Hispanic females (733.2) The chlamydia case rate per 100,000 population for females in 2005 was three times higher than for males (496.5 vs 161.1). Signs and Symptoms Some people may experience a cloudy or yellowish discharge, painful urination, and a dull pain in the abdomen. If left untreated both men and women can become sterile or it can lead to pelvic inflammatory disease in women ( a life threatening infection that affects the lining of the uterus, fallopian tubes, and ovaries). Chlamydia con’t The organisms are found in urethral, cervical, and rectal epithelial cells, but not in exudate. Also, found in throats of women & men having oral sex. The DNA probe is used for both chlamydia and gonorrhea. It can also be detected by urine LCR. Chlamydia & Gonorrhea Gonorrhea is often diagnosed simultaneously with chlamydia-so get treated for both infections upon diagnosis of either one. Partner diagnosis and treatment is important to prevent reinfection and complications. Treatment is the same as for Gonorrhea. Protection against this is provided through the use of condoms. Gonorrhea A reportable disease caused by gramnegative diplococcus Neisseria Gonorrhea. It primarily involves the mucocutaneous surfaces of the GU tract, pharynx, conjunctiva, and anus Purulent discharge can be noted in men (called the drip or clap) Meanwhile, up to 80% of women are asymptomatic. Pathophysiology The most common clinical presentation is an infection of the lower genital tract; which primarily manifests as male urethritis (the drip) and female endocervicitis (inflammation of the mucous lining of the uterine cervix). Infection of the pharnyx, rectum, and female urethra occur frequently but are more likely to be asymptomatic or minimally symptomatic. Gonorrhea This is a curable disease of the penis, butt hole, lining of the eyelid, and the throat Even if your partner doesn’t ejaculate (cum), the gonorrhea bacteria can still be present Although some men show no symptoms-others may experience- yellow-white d/c from penis, pain when defecating, increased voiding and pain or swelling of their scrotal sac. Gonorrhea infections in the mouth & throat usually present w/no symptoms or as pharyngitis. Who is at risk for Gonorrhea? Young sexually active individuals Non-white urban poor Those engaged in high risk behaviors such as drug use, prostitution, and/or multiple partners On the rise in gay and bisexual men Highest rates in females ages 15-19y/o and males 20-24y/o **Up to 50% of those w/gonorrhea have a coexistent chlamydia infection Untreated Gonorrhea Untreated gonorrhea can also result in disseminated gonococcal infections to the ophthalmia neonatorium in newborns (a form of conjunctivitis mostly contracted during delivery by an infant whose mother is infected with gonorrhea), and it can lead to blindness unless promptly treated. *Infections caused by gonorrhea are a major cause of PID, ectopic pregnancy, and chronic pelvic pain. Epididymitis This is a complication resulting from the spread of a gonococcal infections to the posterior urethra that can lead to infertility if left untreated. Gonorrhea, Epididymitis Syphilis Syphilis is a complex sexually transmitted disease (STD) caused by the bacterium Treponema Pallidum. It has often been called the great imitator because so many of the signs and symptoms are indistinguishable from those of other diseases. The syphilis bacterium is passed from person to person through direct contact with a syphilis sore. Sores mainly occur on the external genitals, vagina, anus, or in the rectum. Sores can also occur on the lips or in the mouth. Pregnant women can pass it to their babies How syphilis is not spread? Syphilis cannot be spread by: toilet seats door knobs swimming pools, hot tubs, or bath tubs Sharing clothing, and/or eating utensils. Syphilis The time from first exposure to the bacteria and signs and symptoms can range from 10 to 90 days (average 21 days). The primary stage is marked by the appearance of a single sore (called a chancre). The chancre is usually firm, round, small, and painless. It appears at the spot where the bacterium entered the body. The chancre lasts 1-5 weeks and will heal on its own, if adequate treatment is not administered, it progresses to the secondary stage. Primary stage of syphilis-picture Syphilis 1st Stage Secondary stage con’t The 2nd stage starts when one or more areas of the skin break into a rash that usually does not itch. Rashes can appear as the chancre is fading or can be delayed for weeks. The rash often appears as rough, copper penny spots on both the palms of the hands and soles of the feet. The rash may also appear as a prickly heat rash, small blotches, or scales all over the body, as a bad case of old acne, as moist warts in the groin area, as slimy patches in the mouth, as sunken circles the size of a nickel or dime, or as pus filled bumps that look like chicken pox. Secondary stage The Third Stage (Latent) This stage of syphilis begins when the secondary symptoms disappear. If the infected person has not received treatment, he/she still has syphilis. The bacterium remains in the body and begins to damage the brain, internal organs, nerves, the eyes, heart, blood vessels, liver, bones, and joints. rd 3 stage Latent Stage Syphilis Con’t Late stage signs and symptoms include not being able to coordinate muscle movements, paralysis, no longer feeling pain, gradual blindness, dementia (madness), repeated vomiting, or other personality changes. Men may also experience impotence, and others may feel shooting pains, have blockage or ballooning of the heart vessels, tumors on the skin, bones, liver or other organs, damage to knee joints, and deep sores. Viral infections Herpes- painful open sores Genital wartscaused by Human Papilloma Viruscauses painless cauliflower like warts Hepatitis B- if it does not clear will develop into a chronic infection HIV- Human Immunodeficiency Virus Herpes (HSV) It’s an infection caused by the Herpes Simplex Virus Since it’s a virus, drugs like antibiotics can’t be used to cure it. Oral herpes- is caused by herpes simplex virus type 1- commonly causes cold sores or fever blisters that appear on or around the mouth Genital Herpes- caused by HSV type 2 Blisters appear on or around the sexual organs exposed to the fluids or sores Herpes Transmission Oral herpes is transmitted by kissing someone who has active sores around the mouth Genital herpes- is usually transmitted through sex or genital contact with someone who has active sores in the genital region, or it can be transmitted at the skin surface when the virus is active. (i.e., it can be transmitted without active sores present, this is called-viral shedding) Herpes Symptoms Sores appearing singly or in clusters are the primary symptoms, and they can be painful or painless Swollen glands around the groin or neck may be present during the first outbreak Flu-like symptoms- such as fever, muscle aches, and a sick feeling are common during the first episode Pain in the genital area during urination and intercourse is also sometimes noted Genital Warts/HPV Genital warts are caused by a group of viruses called HPV ( or Human Papilloma viruses) It’s spread by sexual contact during vaginal, anal, or oral sex. The shape and location of the genital warts may vary. In addition to the genital area, they may occur in the anal or rectal area and even the throat. HPV Slide HPV in the mouth Genital Warts Con’t Genital warts can be dangerous (i.e., certain types are linked to cervical cancer as well as other types of cancers in women and men). Genital warts are highly contagious- they may appear single or in clusters, be pink, or red flesh in color, be flat or raised, and sometimes difficult to see with the naked eye (detected with Pap/Colposcopy) Treatment for HPV Podophyllin- applied to the warts and can be used for more than one application Freezing- Cryosurgery- uses cold liquid- like liquid nitrogen Laser Surgery- high intensity light is used to destroy both cervical and skin warts TCA- (Trichloracetic Acid)- this is a powerful acid that can destroy stubborn warts Electrosurgery- an electric needle is used to burn off warts under a local anesthetic HPV Vaccine As a means of combating the rise in cervical cancer rates, a vaccine has been developed to reduce HPV transmission. It can be administered to young girls bet. the ages of 926. The injections 0.5ml IM are given at 0, 2, and 4months after 2nd dose (i.e., 6months). Free through the NJ vaccine program for those under 18 or 18 and older with first injection while in H.S. Merck has patient assistance program for those 26 & under who have or have not contracted HPV, or those with cervical dysplasia interested in taking the vaccine. Hepatitis B HBV virus is a DNA virus In North America & Europe, Hep B is most common amongst adolescents and young adults. Usually spread via sexual contact & percutaneous (needle) exposure. Severity of infection ranges from asymptomatic to fulminant w/fatal liver failure. It can progress to chronic liver disease w/cirrhosis or to the development of hepatocellular carcinoma (cancer). HBV- where’s it found? & How’s it Transmitted HBV can be found in blood, tears, cerebrospinal fluid, breast milk, saliva, vaginal secretion and seminal fluid HBV is transmitted parenterally, via sexual contact, and perinatally Heterosexual contact is the most common mode of transmission, followed by IV drug use, homosexual activity, and transmission from mother to child at time of birth. Not transmitted by fecal-oral route HIV covered under separate lecture Some good news… After increasing 23 percent between 1972 and 1990 (including 10 percent between 1987 and 1990), the teen pregnancy rate for girls aged 15-19 decreased 28 percent between 1990 and 2000 to a record low. 120 116.9 115 111.0 110 105 100 106.7 99.6 95 90 85 83.6 80 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 Henshaw, S. (2003). U.S. teenage pregnancy statistics with comparative statistics for women aged 20-24. New York: The Alan Guttmacher Institute. Why Care about Subsequent Births Overall teen birth rates are down, but additional births to teen mothers are still disturbingly common. In 2002, there were nearly 89,000 such births, representing 21% of all teen births. Nearly 1/4 of teen mothers have a second birth before age 20. Additional Births Reasons for second births are less apparent than first births. Causes of first births (un-realistic view of motherhood, lack of knowledge of contraception, it can’t happen to me), presumably do not apply to women who are already teen mothers. What Research Shows: Age Studies Some differ on the importance of age. non-nationally representative studies suggest that having a child at a younger age increases the chance of a second birth during the teen years. What Research Shows: Race/Ethnicity The difference in rates of second births overall does not significantly vary by race/ethnicity. African-American and Hispanic/Latina teen mothers were slightly more likely than White teen mothers to have closely spaced second births. What Research Shows: Education Lower educational expectations are associated with having additional births. Dropping out of school before or after first birth was associated with a greater risk of having a second child as a teen and close spacing between births. Girls with low cognitive ability are almost three times more likely to have a second birth as a teen than those with high cognitive ability. Consequences: Teen Mothers Medical: Teen mothers initiate pre-natal care later with subsequent pregnancies. Education: Additional births make the teen mother less likely to attend school or to complete school. Work: Additional births make it less likely that a teen mother will be working and more likely that they will be on welfare. Consequences: Children Five years postpartum, children of teen mothers who had avoided additional births were: Better prepared for school Better behaved More outgoing and happy The spacing between births seems to be the most important factor because of how it affects time devoted to first child. References Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines 2005. MMWR 2002; 51(no. RR-6). http://www.cdc.gov/std/chlamydia/STDfactChlamydia.htm http://www.cdc.gov/std/syphilis/STDFactSyphilis.htm