Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
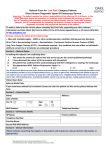
Print Form Peter MacCallum Cancer Centre REFERRAL FORM Sign completed referral forms and fax to (03) 8559 7371 or email to [email protected] Patient details: Referral Date: Last name: Medicare eligible: First name: D.O.B: Yes No Yes No Medicare number: Sex: Appointment requirements: Address: - Interpreter required: If yes, language required: Preferred contact phone number: - Accommodation assistance required: Email address: Yes No Please select the services you wish to refer the patient to: If unsure of which service to refer, please select "All services". All referrals receive multidisciplinary assessment and will be promptly triaged to the most appropriate service (e.g. Breast, Lung) and clinician. ✔ All services - Prof A. Heriot, Prof D. Rischin, A/Prof T. Leong, Prof J. Seymour, Dr P. James Referrals to All services will enable prompt multidisciplinary care if required (recommended) Cancer Surgery (inc skin) - Prof Alexander Heriot Medical Oncology - Prof Danny Rischin Haematology - Prof John Seymour Familial Cancer Centre - Dr Paul James Radiation Oncology - A/Prof Trevor Leong Preferred site (Radiotherapy only) Bendigo Box Hill Moorabbin East Melbourne Sunshine How long is this referral valid? Reason for referral: If requesting a specific clinician, please specify: Indefinite (recommended) 12 months Is this referral for a second opinion? Yes 3 months (Specialists only) No Room for further clinical details available on the second page Relevant investigations/attachments: The tests identified below are to be completed and results fowarded with the referral (tick the relevant boxes) Relevant blood and microbiology results Operation / Scope notes Histopathology report Diagnostic imaging Other: Comments: Referring doctor: Practice name & address: Name: Provider number: Phone No: Please turn page to complete referral Fax No: MANDATORY SIGNATURE: Page 1 of 2 Patient Name: D.O.B: Relevant clinical information: Please include FHx summary for Familial Cancer Centre referrals Past Medical History: Current Medications: Allergies: Page 2 of 2