Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Heart failure wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Aortic stenosis wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
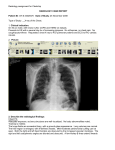
Flow for each: oxygen IV cardiac monitor EKG lab results radiology CPR 30 pumps, 2 breaths 100per minute “Stayin alive” Acute Coronary Syndrome, STEMI Recognize the classic presentation of acute myocardial infarction as well as formulate three additional differential diagnoses consistent with chest pain o Midsternal chest pressure that radiates to left arm w/ SOB, diaphoresis and nausea, not reproduced by palpation o Right arm radiation is most concerning for MI o Abnormal EKG: highest risk for AMI o Myocardial death begins 20 mins after occlusion and complete in 6hrs o DDx: GI issue, anxiety, angina, MSK issue, aortic dissection, arrhythmia -lead EKG with ST segment elevation in precordial leads o EKG: ST segment elevation – coronary vasospasm too o Don’t forget about ST segment elevation in AVR- it’s the widow maker- LCA occlusion o Flipped T in AVL can mean patient is about to have an MI. Institute pharmacologic management for ACS o ACS- manage with LMWH, aspirin, beta blocker o MI protocol: M (morphine) O (oxygen) N (sublingual nitro) A (aspirin) – clopidogril loading does No nitro if hypotensive BP<90) reading an anterior-posterior chest x-ray o Labs: electolytes, ProTime, PTT, cardiac serum markers Troponin 1 o X-ray can look for pulmonary venous congestion / heart could be enlarged and determines risk of thrombolysis per fibrinolytic checklist Recognition and management symptomatic bradycardia according to ACLS algorithm o Is <60bpm-- Atropine (1st line) Dopamine Epinephrine o Transcutaneous pacing if atropine fails (give pt sedation first) o For tachycardia user cardioversion ACS/AMI? o History, ABC’s, IV, O2, cardiac monitor, EKG, Chest X-ray o Fibrinolytic therapy w/I 2-3 hours after onset of symptoms for STEMI (if can’t get to cath lab give clot busting drugs) TPA (tissue plasminogen activator) o PCI safer than clot busting drugs because reduces risk of bleeding in brain Stress test- negative one will decrease risk not eliminate it What is the difference between electrical and mechanical capture when using a transcutaneous pacemaker o Meds for cardioversion are amiodarone for tachycardia! o TECHNIQUE: begin at 10amps and increase in 10amp incriments until pacing noticed at 60-80 o Mechanical capture = rise in BP, pulse, improved color of skin etc Acute MI: leads V2, V3, V5, V6: tombstones (will die if you miss this) Wellens syndrome--- Proximal LAD disease*machine will miss o T-wave abnormality in mid-precordial leads (V2-V3, +V4) o Highly specific for critical obstruction in proximal LAD o High risk for extensive anterior MI, death o 2 patterns: Type 1: more obvious (looks like “W” for wellens) Type 2: see more often but usually misdiagnosed as nonspecific or normal (looks like one sharp vampire tooth and one dull vampire tooth) o Treatment for Wellens Patients best managed w/ cath/PCI, stress testing may precipitate MI (could die!!) Medical management ineffective for proximal LAD lesions (75% will develop AMI w/in weeks) Brugada Syndrome o Associated w/ sudden cardiac death o Individuals usually healthy w/ structurally normal hearts o Can’t treat w/ meds, have to use internal cardioverter-debrillator (AICD) only treatment o Chacterized by--- ECG abnormalities in leads V1-V3--- RBBB or IRBBB pattern Coved Type (most common, pic on right, scary) Saddle Type (picture on left) Transient or permanent ST elevation in V1-V3 Pts w/ prior syncope and ventricular arrhythmias high risk for sudden cardiac death, require ICD Tension Pneumothorax Primary Objectives Understand Tension Pneumothorax is an emergent condition based on clinical findings, not based on radiology/diagnostic findings. o Differentials: Acute coronary syndrome, PE, esophageal rupture, aortic dissection, pericardial tamponade, herpzes zoster (but along dermatome)- rash comes after pain Demonstrate the appropriate landmarks for needle thoracotomy/chest tube insertion o 2nd ICS for tension pneumo mid-clavicular, O2, IV, px meds Needle advanced until air can be aspirated into syringe and needle withdrawn and cannula left open th o 4-5 for regular stable pneumo chest tube site mid- axillary Describe the physical findings associated with Tension Pneumothorax o Trachea deviation, hyper-expanded chest with increased percussion noted, hyperexpanded chest that moves little with respiration o Tachypnea, tachycardia, hypoxic are visible signs Provide causes of pneumothorax, both traumatic and atraumatic o Open (thoracic wall injury) vs closed (alveolar injury/tearing) o Mediastinum shifts toward healthy lung compresses in tension pneumo o Sudden onset of ipsilateral chest/shoulder pain, cough o Tachypnea, unilateral breath sounds (but can be normal w/ small pneumothorax) Pulmonary Embolus & DVTPrimary Objectives Recognize the presentation of Pulmonary Embolus as well as alternative differential diagnoses. o Tachypnea 96%, rales 58%, tachycardia, diaphoresis, lower extremity edema, cyanoses, hemoptysis o Classic are pleuritic chest pain, SOB, hypoxia o DDx: ACS, CHF, pulmomary edema, pneumothorax etc.. Interpretation of 12 lead EKG with features suggestive of acute right heart strain and pulmonary embolus (S1Q3T3 with Right Axis). Tachycardia is the main one Westermark’s sign—focus of oligemia (collapsed vessel distal to the infarct) Interpretation of ABG showing hypoxia and respiratory alkalosis pH>7.45 w/ PaCo2 <35mmHg o Normal PaCO2 is 34-45mmHg o Bicarb normal 22-16mEg/L o PaO2 normal 80-100mmHg is f less then hypoxia Recognition and management of PEA according to ACLS algorithm. –pulseless electrical activity o Problem: wide QRS could be hypoxia or hyperkalemia o Epinephrine IV every 3-5 min and Atropine if bradycardia Iv every 3-5 min o If they go into cardiac arrest can do amiodarone IV What is the mnemonic for the causes of PEA? o MAD (triple H) cat causes of PEA Massive pulmonary embolism, acidosis, drug overdose Hypoxia, hypovolemia, hypokalema/hyper Cardiac tamponade, acute MI, tension pneumothorax Virchow’s Triad: Venous Stasis endothelial damage hypercoagulability DVT: thrombus in a deep vein (lower extremity) o Well’s Criteria Active cancer calf swelling, collateral superficial veins Paralysis, paresis, recent immobilization of LE, bedridden w/in 3 days or surgery w/in 3 months Pitting edema in involved leg Alternate diagnosis more likely -2 Scoring: 3 or more risk factors: high risk: 60-75% 1-2 risk factors: moderate risk: 17-38% 1 or less: low risk: 3-13% o Detection D-dimer (sensitive for ongoing fibrinolysis, but not specific for thrombosis Contrast Venography* gold standard Venous Ultrasonography: checks compressibility of veins PE: emboli lodges from leg usually pulmonary a. o Well’s Criteria Clinical S/S of DVT (risk of PE) PE more likely diagnosis or equally likely HR >100 Immobile >3 days or surgery w/in past 4 weeks Previous DVT or PE (recur) Hemoptysis Malignancy (very hypercoagulable) Scoring >6 points: high risk 2-6 points: moderate risk <2 point: low risk o Diagnosis D-dimer: do if low/moderate risk of Well’s Criteria troponin (mild elevation) and echo- R. heart strain CXR: larger PE: Hamptons hump CT chest w/ contrast: modality of choice Looking for filling defects, centralt o periphery Have to have working kidneys, radiation V/Q scan o Treatment Heparin: first line therapy as IV continuous form, safe in preggers Coumadin: inhibits Vit K dependent factors: requies heparin overlap, requires INR If first time reversible event (surgery/trauma)- continue Coumadin/Heparin for 3 months If first episode idiopathic: 6 months Recurrent idiopathic or continuing risk factor: 12 months Thrombolysis/tPA for massive PE or unstable VS Cateter embolectomy Thrombectomy/embolectomy: surgical excision (rare, high mortality) Thoracic Dissection Primary Objectives Recognize the classic presentation of thoracic aortic dissection as well as formulate three additional differential diagnoses consistent with chest pain o Biggest risk factor is HTN (marfan, Ehlers danlos, weight lifting increase risk too) o DDx: myocardial infarction, pulmonary embolus, aortic aneurysm Verbalize the findings of ST elevation on 12-lead EKG as it relates to thoracic aortic dissection o The EKG in most patients with aortic dissection is either normal or shows only nonspecific ST-T changes. Identify varying blood pressure readings in the upper extremities as a clue to Thoracic Dissection o A pulse deficit or >20mmHg difference in BP between the right and left arm Interpret the chest x-ray consistent with widened mediastinum Interpret the Chest CT showing thoracic aortic dissection Recognize that Thoracic Aortic Dissection is a surgical emergency requiring immediate intervention by a cardiothoracic surgeon and that blood pressure control is vital with Esmolol and Nitroprusside Sodium Nitroprusside give w/ BB to not HR o Debakey Classification: used most often Debakey I: ascending, arch and descending origin Debakey II: ascending aorta origin Debakey III: originates in descending aorta, can extend proximal/distally o Stanford A: Ascending aorta: more common and more lethal (A’s go together) Anterior chest pain more common (ascending aorta) o Standford B: does not involve ascending aorta (B for Bubba- because you usually see this in older, heavy men w/ HTN) Back pain more common (desceding aorta) Pulse deficit **check all 4 pulses in chest pain cases and get BP in both arms** Acute if less than 2 weeks Abrupt onset of chest pain described as “ripping or tearing” and “radiating to back” Neck and jaw pain= aortic arch Syncope: bad sign: poor prognosis Anyone >50 w/ syncope and any pain= think dissection Neurological symptoms (could mimic stroke) Can’t give tPA for dissection!! could bleed out! Traumatic Dissection o Other signs include L. apical hematoma (apical capping), fracture of 1st or 2nd rib, scapula, or sternum (blunt trauma), deviation of NG tubes, ET tube or trachea to right o Can be from rapid deceleration (fall) or high speed MVA, majority occur at aortic isthmus o Aortic Injury Grading Type I: Intimal tear Type II: intramural hematoma Type III: pseudoaneurysm Type IV: rupture Diagnosis Abrupt onset of thoracic or abd pain w/ sharp, tearing, or tipping character o Mediastinal and/or aortic widening on CXR o Variation in pulse and/or BP (>20mmHG difference between arms) o Transesophageal echo: diagnosis of choice!! o Cat scan (CTA) best for traumatic aortic injury Congestive Heart Failure Primary Objectives Recognize the classic presentation of CHF as well as formulate three additional differential diagnoses consistent with chest pain o Acute Sx: palpitations, sudden severe dyspnea, cough up pink/white foam/throathy mucus, chest pain (if caused by HA), jugular venous distention o Chronic Sx: Dyspnea, weakness, swelling, irregular heartbeat, cough/wheezing, ascites, o DDx: Pulmonary embolism, Pneumonia (including aspiration), COPD exacerbation, Reactive airway disease exacerbation (Wheezing may be present in asthma/RAD and pulmonary edema), MI, pulmonary edema o Most common etiology of systolic and diastolic heart failure in the United States is coronary artery disease Interpret 12-Lead EKG with sinus tachycardia with LVH and ventricular ectopy o LVH EKG: wide QRS; ST in opposite direction of QRS and T wave inversion o Vencticular ectopy: also called premature ventricular contractions or PVCs, can be caused by cardiomyopathy, feels like a skipped beat and seen on Holter monitor More PVCs in a row becomes ventricular tachycardia o Kerley b lines from pulmonary edema o w/ cephalization Blunted costophrenic angle – from pleural effusion cardiomegaly Understand the use of non-invasive respiratory support of CPAP/BiPAP in the management of acute CHF o Both are positive airway pressure o CPAP is continuous and you can set a level to give pressure and keeps the upper airway open respiratory issues o BPAP can set bilevels of pressure with inspiratory and expiratory pressures used for respiratory issues and heart disease Interpret laboratory results of the B natriuretic peptide and its use is diagnosing pulmonary edema o Low levels of BNP (<100 pg/ml) suggest a cardiac cause is unlikely o BNP is secreted by the ventricles of the heart in response to excessive stretching of heart muscle cells Manage acute CHF with nitrates and diuretics and understand the mechanism by which these pharmacologic agents act o Nitrates: coronary vessels improves oxygen supply to the myocardium. The dilation of peripheral veins, and in higher doses peripheral arteries, reduces preload and after-load, and thereby lowers myocardial oxygen consumption. o Diuretics: increase urinary sodium and water loss – used for edema and HTN Secondary Objectives: What are the ACLS treatment guidelines for the management of ventricular fibrillation? CPR until defibtrillater attatched to patient using 120-200joules CPR resumed for 5 cycles between each shock, check heart rhythm in between To ensure safety during the shock, providers should always announce the following statement, “I am going to shock on three. One, I’m clear…Two, you’re clear…Three, everybody is clear.” Vasopressor Epinephreine is given to constrict blood vessels (increases BP too) Amiodarone can be used for antiarrhythmic Diastolic Dysfunction • Abnormal (LV) cardiac relaxation and filling and/or cardiac stiffness, with elevated LV filling pressures • Preserved (LV) ejection fraction >50% (ECHO) • Underlying causes : Ischemic heart disease (coronary artery disease), Atrial fibrillation, Hypertension, Hypertrophic obstructive cardiomyopathy (HCM/HOCM), Restrictive cardiomyopathy Treatment • Control hypertension •BB/ CCB (diltiazem) Control heart rate, especially with atrial fibrillation •Diuretics (furosemide) and nitrates Maintain volume status and decrease preload Systolic Dysfunction • Impaired left ventricular contractile function • Ejection fraction <50% (ECHO) • Underlying causes: Ischemic heart disease (coronary artery disease), Idiopathic dilated cardiomyopathy, Hypertension, Valvular heart disease Treatment • Diuretics (furosemide) •ACE inhibitors or angiotensin II receptor blockers (ARBs) Afterload reduction •Beta blockers (carvedilol, metoprolol, bisoprolol) •Spironolactone •Nitrates and Hydralazine New York Heart Association (NYHA) Classification • Class I: Symptoms of heart failure at activities that would limit normal individuals • Class II: Symptoms of heart failure with ordinary exertion • Class III: Symptoms of heart failure with less than ordinary exertion • Class IV: Symptoms of heart failure at rest*** • Approximately 50 to 75% of patients with heart failure have coronary artery disease General Treatment: Treat coronary artery disease and risk factors: Diabetes, Hypertension, Hyperlipidema , Smoking cessation, Restore coronary perfusion with stent placement or CABG, as indicated Implantable Cardioverter Defibrillator (ICD) for severe or VT going to VF Cor Pulmonale-- Altered structure and/or function of the right ventricle that results from elevated pulmonary artery pressure (pulmonary hypertension) Things to note on the SIM dudes: Wear gloves at all times Airway: cyanosis notes by blue intensity of LED in mouth, can do endotracheal intubation and surgical airway Circulation: pulses at coritd, radial, femoral, dorsalis pedia, anterior tibial IV attempts with venous access pad ; Fluids—tears, sweat, blood Larger snaps for hands free defibrillation and transcutaneous pacemaker cables: Smaller snaps are for cardiac monitor limb leads on shoulder and lower abdomen Sounds: 4 heart sounds, 5 lung sounds, 2 bowel sounds; Pupils accommodate and respond to light w/ eyes for alertness Monitor: HR (green), PulseOx (yellow), BP (red), CO2(purple), Temp (green), Pulse (yellow) and RR (purple)