Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Marginalism wikipedia , lookup
Surplus value wikipedia , lookup
History of macroeconomic thought wikipedia , lookup
Icarus paradox wikipedia , lookup
Production for use wikipedia , lookup
Microeconomics wikipedia , lookup
Brander–Spencer model wikipedia , lookup
Theory of the firm wikipedia , lookup
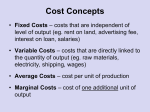
Economics of health care Topic 10. Health care providers as firms 1. Theory of the firm: profit maximisation, price, quantity and costs. Perfect competition: industry equilibrium Each firm is a ‘price taker’ MR = the addition to revenue resulting from a 1 unit increase in quantity sold. MR the same over all Qs Profit maximising quantity is where MC = MR. Imperfect competition: Each firm faces a downward sloping demand curve MR schedule also downward sloping Profit maximising quantity is where MC = MR. The price which will be charged at that quantity will be ‘read off’ the demand curve 2. Why are hospitals different? Services are produced ‘at the point of demand’; cannot be stored; poorly substitutable between patients. In contrast to other firms, decisionmaking highly decentralised; individual workers (Drs) have discretion over resource use. Provision is dominated by not-for-profit (nfp) firms profit maximisation may not be the appropriate maximand. 3. Why do not-for-profit firms exist? Weisbrod (1975): satisfies demands for goods in which markets fail (externalities, public goods) Hansmann (1980): a response to contract failure (where quantity/quality of output not easily observed by the purchaser) Bays (1980): interest group theory. (for a useful review of each, see Folland Goodman and Stano). Theories of hospitals as firms a. ‘traditional’ theory of the firm: profit maximisation b. Managerial theories of the firm: hospital pursues other (or multiple) objectives c. Behavioural theories: internal bargaining between rival groups within the hospital, rather than the specification of an objective function. (a) a priori not applicable to nfp (b) & (c) could apply to fp and nfp 4. Maximisation of quantity (Baumol 1967) P MC AC D Q1 MR Q2 Quantity of patient days Profit max = Q1 Quantity max = Q2 (where AC = Average revenue) subject to a ‘breakeven’ profit constraint. Q is higher than profit maximisation would predict and prices are lower 5. Maximisation of quality (Lee 1971) Managers of n-f-p maximise utility by attempting to enhance the status/prestige of their institutions. Managerial utility = f(salary, security, power, status) Status positively related to the range of services available and the extent to which expensive and highly specialised equipment and doctors are available. Suggests higher costs May explain duplication of resources and overspecialisation? 6. Maximisation of quantity & quality (Feldstein 1971; Newhouse 1970) Managers choose a combination of quality and quantity that maximises their utility. Given a trade-off between quantity and quality, managers will seek an optimal combination of the two to produce. P, AC AC3 AC2 AC1 Q1 Q3 Q2 quantity quality quantity 7. The managerial discretion model (Williamson 1963) A model developed to explain the behaviour of large firms not directly managed by major shareholders Asymmetry of information between shareholders and managers about the performance of the firm. Managers will choose the profit maximising output and price But will absorb profits through discretionary expenditures (increasing wages, staff, prestige; utility-enhacing) 8. The hospital as a physicians’ cooperative Pauly and Redisch (1973) The objective function is the maximisation of pecuniary gain to the ‘decisive’ set of decision makers. The hospital is de facto controlled by the doctors, who operate the hospital so as to maximise their net incomes. NR/M = (P.Q – rK – wL)/M Physicians’ income max Supply Net average revenue Number of staff physicians 9. The hospital as ‘two firms in one’ (Harris 1977) separation of supply and demand functions Drs, as agents for the patient, demand services from other hospital staff (lab, pharms, nurses, blood supply) Institutional constraints that arise through the medical and ethical motives of Drs, as opposed to their economic motives, that are important. “…it should be understood that the organisation is set up to protect the Dr from behaving as an economic man” 10. Research evidence The performance of for-profits vs. not-forprofits theory suggests f-p hospitals will be more efficient. Evidence on this is of interest because… in the UK, greater use of the private sector in the US, conversion from n-f-p to f-p status Sloan (1988) “Empirical evidence reveals little or no difference in efficiency of ownership type”. implications for competition between f-p and n-f-p?