Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
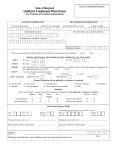
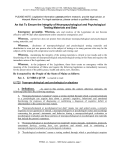
Psychological or Neuropsychological Testing Request Questions? Please call us at 1-800-345-6784 Member Name: Subscriber ID Number: Member DOB: Phone: ( ) Gender: Age: Referring Provider Name, Credential: Male Female Tax ID #: Referring Provider Street Address: Referring Provider City: State: Referring Provider E-mail Address: Phone: ( ) ZIP: Fax: ( Referring Provider’s Role with Member (e.g., PCP, Therapist, etc.): Form completed by: Provider Administering Tests Name, Credential: Tax ID #: ) Testing Provider Licensure (if not a psychologist, include credentials for performing psychological testing): Testing Provider Street Address: Testing Provider City: State: Testing Provider E-mail Address: Place of Service: Phone: ( ) ZIP: Fax: ( ) Inpatient Facility. If checked, name of facility: Psychologist’s Office Outpatient Treatment Center Other—Describe: Complete to the best of your knowledge including the current, provisional and/or rule out diagnosis for each axis. AXIS DIAGNOSIS DSM IV Code Description Axis I: Axis I: Axis II: Axis II: Axis III: Axis III: CLINICAL INFORMATION Relevant clinical history including current, specific presenting symptoms that support testing request: What question(s) is psychological testing expected to answer and how will the test results influence treatment? Medications: Anti-Depressants Anti-Psychotics Other: Is patient currently abusing any substances? Anti-Convulsants Anti-Anxiety Agents Mood stabilizers other than anti-psychotics and anti-convulsants Yes No If Yes, describe: Unless specifically requested elsewhere in this document, please do not send a DNA or other genetic sample, or the results of any genetic typing, test or analysis, including DNA. Confidentiality Notice: The information contained in this facsimile message is privileged or confidential, and intended only for the individual or entity named above. If the reader is not the intended recipient, or the employee or producer responsible to deliver it to the intended recipient, you are hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited. If you have received this communication in error, please immediately notify us by telephone at the number listed on this page. 020957 (09-2009) Page 1 of 2 An Independent Licensee of the Blue Cross Blue Shield Association REQUESTED TEST(S) DETAILS Member Name: Subscriber ID Number: Type of Testing: Psychological Neuropsychological Please list or attach list of all proposed tests. For test batteries (e.g., HRNB), list specific subtests of batteries. Test Name(s): TESTING DATES DISTRIBUTION OF HOURS Psychological Testing CPT Code 96101 Neuropsychological Testing Time CPT Code 96116 96102 96118 96103 96119 Other: 96120 Time Total hours of testing requested: 90801 Initial Evaluation Interview Needed? Yes No For CPT Codes 96102 and 96119, please indicate the licensure of the technician or confirm that the technician will be supervised by a licensed mental health provider whose scope of practice includes psychological testing: Note: If testing has already been completed, include a copy of the typed testing report. Initial Evaluation Date: Testing Date(s): Feedback Session Date: Provider Signature: X Date: E-mail this request to: [email protected] Note: If this is your first e-mail submission, log onto https://voltage-pp-0000.premera.com/login and create a secure e-mail account. Or fax to: 1-800-843-1114 or 1-888-704-2091 Or mail this request to: Premera Blue Cross Attention: Behavioral Health P.O. Box 34299, MS 438 Seattle, WA 98124-1299 Questions? Please call us at 1-800-345-6784 Unless specifically requested elsewhere in this document, please do not send a DNA or other genetic sample, or the results of any genetic typing, test or analysis, including DNA. Confidentiality Notice: The information contained in this facsimile message is privileged or confidential, and intended only for the individual or entity named above. If the reader is not the intended recipient, or the employee or producer responsible to deliver it to the intended recipient, you are hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited. If you have received this communication in error, please immediately notify us by telephone at the number listed on this page. 020957 (09-2009) Page 2 of 2 An Independent Licensee of the Blue Cross Blue Shield Association