Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
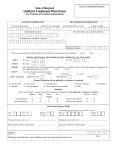
Outpatient Treatment Report Provider Name & License/Certification Type (Please Print): 6588 Member Name (Please Print): ___________________________________________ _________________________________________ NPI: Member ID #: Tax ID #: / DOB: CPT Codes Requested Numeric Code-Modifier / Diagnoses Axis II: Axis I: . Axis I: GAF: . Axis III: . CPT: Sometimes- CPT: - Check box if member has been previously hospitalized. . Axis IV:__________________________ List Medications Below: ______________________ ______________________ ______________________ Check box if member is pregnant. Provider Signature:_________________________________ Date Signed: FUNCTIONAL IMPAIRMENT RATING SCALE Fill in the bubble like this of impairment in each domain. Medications Anti-depressant Anti-psychotic Anti-anxiety Mood Stabilizer Sleep Aid ADHD Medication Other to indicate current level / CURRENT LEVEL OF IMPAIRMENT None Moderate Affective Depression, mania, mood instability, inappropriate mood Anxiety Panic, worry, anxiety, easily startled, flashbacks, nightmares ADHD Symptoms Hyperactivity, impulsivity, poor insight, poor judgment Obsessions & Compulsions Rituals, fear of contamination, excessive need for orderliness, hair pulling, unacceptable impulses Reality Construction & Thought processes Delusions, hallucinations, disorganized or racing thoughts, dissociative states, paranoia Cognitive Cognitive impairments due to organic conditions including brain trauma, dementia and mental retardation Social Difficulty forming positive relationships, social isolation, anger/aggression, interpersonal problems at work/school Substance Abuse Problematic use of drugs or alcohol Harm to Self or Other Suicidal ideation, intentionally self injurious behavior, suicide planning, danger to others Appetite & Eating Disturbances in appetite, anorexia or bulimia Sleep Disturbances in sleep patterns, including excessive sleep Other Medical Conditions Presence of medical conditions which have significant impact on patient functioning and/or quality of life 500 Fax Completed Forms To: 877-675-7421 Provider Secure Fax #: (Required) / State: (Required) Severe