Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
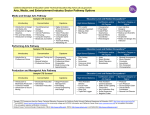
Rectal Cancer Treatment Pathway Disease Pathway Management Secretariat Version 2013.5 Disclaimer The Rectal Cancer Treatment Pathway (Pathway) is intended to be used for informational purposes only. While the Pathway represents an overview of the treatment of a typical rectal cancer, it is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all treatments are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the Pathway. Rectal Cancer Treatment Pathway Pathway Preamble Pathway Disclaimer The Rectal Cancer Treatment Pathway (Pathway) is a resource that provides an overview of the treatment of a typical rectal cancer. The pathway is only intended for primary adenocarcinoma and familial cancers (Lynch/non-Lynch) and cancers complicating inflammatory bowel disease are handled differently. The information contained in this Pathway is intended for healthcare providers and other stakeholders in the cancer system, including administrators and organizers. The Pathway is intended to be used for informational purposes only. While the Pathway represents an overview of the treatment of a typical rectal cancer, it is not intended to constitute or be a substitute for medical advice and should not be relied upon in any such regard. Further, all treatments are subject to clinical judgment and actual practice patterns may not follow the proposed steps set out in the Pathway. The Pathway is not intended for patients. In the situation where the reader is a patient, the reader should always consult a healthcare provider if he/she has any questions regarding the information set out in the Pathway. The information in the Pathway does not create a physician-patient relationship between CCO and the reader. Version 2013.5 Page 2 of 7 Pathway Legend Primary Care Provider (Family Physician, Nurse Practitioner, Emergency Department Physician) Endoscopist Pathologist Diagnostic Assessment Program (DAP) Surgeon Radiation Oncologist Medical Oncologist Imaging Multi-disciplinary Cancer Conferences (MCC) Palliative Care and Psychosocial Oncology Team While care has been taken in the preparation of the information contained in the Pathway, such information is provided on an “as-is” basis, without any representation, warranty, or condition, whether expressed, or implied, statutory or otherwise, as to the information’s quality, accuracy, currency, completeness, or reliability. CCO and the Pathway’s content providers (including the physicians who contributed to the information in the Pathway) shall have no liability, whether direct, indirect, consequential, contingent, special, or incidental, related to or arising from the information in the Pathway or its use thereof, whether based on breach of contract or tort (including negligence), and even if advised of the possibility thereof. Anyone using the information in the Pathway does so at his or her own risk, and by using such information, agrees to indemnify CCO and its content providers from any and all liability, loss, damages, costs and expenses (including legal fees and expenses) arising from such person’s use of the information in the Pathway. Pathway Considerations § § § The family physician should be informed of all tests and consultations. Usual ongoing care with the family physician is assumed to be part of the Pathway. Clinical trials should be considered for all phases of the Rectal Cancer Treatment Pathway, where available. All patients under consideration for an ostomy should be referred to an Enterostomal Therapy Nurse preoperatively. Patients should have access to an Enterostomal Therapy Nurse before and after ostomy surgery. Ostomy Care and Management, Clinical Best Practice Guideline, Registered Nurses Association of Ontario. No Specific Specialist Designated Possible Action or Result Referral to Managing Physician at Pathway Entry Point Pathway Target Population Patients with a confirmed rectal cancer diagnosis who have undergone the recommended diagnostic and staging procedures as outlined in the Colorectal Cancer Diagnosis Pathway. Rectal Cancer Treatment Pathway Stage 0 Version 2013.5 Page 3 of 7 Stage 0 Tis | N0 | M0 AJCC Cancer Staging Manual 7th edition. Endoscopist (Surgeon or Gastroenterologist) Polypectomy or Local Excision Pathology Review Pathology Report Histopathology confirms stage 0 and complete resection Colonoscopy Surveillance Refer to Guidelines for Colonoscopy Surveillance After Polypectomyα α To complement the colonoscopy standards, CCC adopted these surveillance guidelines: Guidelines for Colonoscopy Surveillance after Polypectomy: A consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society. Gastroenterology 2006; 130:1872-1885 Rectal Cancer Treatment Pathway Stage I Rectal Cancer AJCC Cancer Staging Manual 7th edition. Polypectomy Pathology α To complement the colonoscopy standards, CCC adopted these surveillance guidelines: Guidelines for Colonoscopy Surveillance after Polypectomy: A consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society. Gastroenterology 2006; 130:1872-1885 Review Pathology Report Histopathology: - Cannot confirm complete resection margins (negative margins are the goal of resection; can consider further endoscopic resection) OR - Unfavourable histopathological features (e.g., poorly differentiated or undifferentiated, lymphovenous invasion) Enterostomal Therapy Nurse Endoscopist (Surgeon or Gastroenterologist) Total Mesorectal Excision with Low Anterior Resection or Abdominoperineal Resection Refer to EBS #17-4 Proceed to the Colorectal Cancer Follow-up Care Pathway Pathology Refer to EBS #17-4 Review Pathology Report Radiation Oncologist MCC Radiation Oncologist Review Pathology Report Biopsy Pathology NOTE: Early referral to psychosocial oncology and palliative care team is recommended Radiotherapy or Chemoradiotherapy Medically Inoperable (e.g., medically unfit for surgery) Medical Oncologist Local Surgical Management Adjuvant (Postoperative) Therapy Chemotherapy Pathological Stage II or III Surgeon Page 4 of 7 Colonoscopy Surveillance Refer to Guidelines for Colonoscopy Surveillance After Polypectomyα If histopathological features confirms complete resection Stage I T1 | N0 | M0 T2 | N0 | M0 Version 2013.5 Medical Oncologist And/ Or Chemoradiotherapy Proceed to the Colorectal Cancer Follow-up Care Pathway Rectal Cancer Treatment Pathway Rectal Cancer Stage II and III Version 2013.5 Page 5 of 7 NOTE: EBS #2-4 is older than 3 years old and is UNDER REVIEW for currency and relevance. Stage II Stage IIA T3 | N0 | M0 Stage IIB Referrals for Preoperative Therapy T4a | N0 | M0 Preoperative Chemoradiotherapy Refer to EBS #2-4 Stage IIC Resectable T4b | N0 | M0 Radiation Oncologist Stage III Medical Oncologist Preoperative Hypofractionated Radiotherapy Alone Refer to EBS #2-4 Stage IIIA T1,T2 | N1/N1c | M0 T1 | N2a | M0 Stage IIIB T3-T4a | N1/N1c | M0 T2-T3 | N2a | M0 T1-T2 | N2b | M0 Stage IIIC T4a | N2a | M0 T3-T4a | N2b | M0 T4b | N1-N2 | M0 Managing Physician from diagnosis and staging Enterostomal Therapy Nurse Pathology Refer to EBS #17-4 Adjuvant Chemotherapy Refer to EBS #2-4 If un-resectable Palliative Chemotherapy Refer to EBS #17-4 MCC If resectable MCC Guidelines and Resources AJCC Cancer Staging Manual 7th edition. Total Mesorectal Excision with Low Anterior Resection or Abdominoperineal Resection Goal is to achieve clear margins Radiation Oncologist Medical Oncologist Radiation Oncologist Medical Oncologist Chemoradiotherapy Re-evaluate at MCC Potentially downstage to make resectable Re-evaluate resectabilIty (ongoing process). Allow adequate time for downstaging. Consider planning for more extensive surgery if required (e.g., pelvic exenteration) Unresectable NOTE: Early referral to psychosocial oncology and palliative care team is recommended Palliative Radiation with or without Chemotherapy Proceed to the Colorectal Cancer Follow-up Care Pathway Rectal Cancer Treatment Pathway Rectal Cancer Stage IV EBS #2-25 is older than 3 years old and is UNDER REVIEW for currency and relevance. Stage IV Multidisciplinary Referrals to Create Individualized Care Plan Stage IVA Any T | Any N | M1a Stage IVB Any T | Any N | M1b AJCC Cancer Staging Manual 7th edition. Surgeon* Sequence of care is individualized and is dependent on symptomology and resectability. Managing Physician from diagnosis and staging MCC Evaluate for resectability of primary and of metastatic disease Symptomatic primary must be dealt with initially MCC Guidelines and Resources NOTE: All patients under consideration for an ostomy should be referred to an Enterostomal Therapy Nurse preoperatively. Patients should have access to an Enterostomal Therapy Nurse before and after ostomy surgery. Evaluate Metastatic Disease Neoadjuvant Chemo-radiotherapy (neoadjuvant radiation is preferred over an adjuvant approach) Resection of Primary Neoadjuvant Chemotherapy *Opinion from a surgeon with relevant expertise should be obtained (e.g., Hepatobiliary or thoracic surgeon) NOTE: Early referral to psychosocial oncology and palliative care team is recommended Resection of metastatic liver lesion(s) Radiation Chemotherapy Refer to EBS #2-25 Primary tumour requires treatment even if asymptomatic. Primary Tumour Unresectable If metastatic disease is resectable, downstaging pelvic disease to resectable could be considered Re-assess metastatic lesion(s) Appropriate Palliative Therapy may include one or more of the following: Unresectable Metastatic Disease** Medical Oncologist Page 6 of 7 Care is individualized. Items discussed and considered at the MCC: § Sequencing of primary and metastatic disease resection § Synchronous vs. staged approach for resection The sequence of care presented below is a possible approach, however it may vary. Refer to EBS #17-7 Radiation Oncologist Palliative Care & Psychosocial Oncology Team **Individuals with oligo-metastases who are not surgical candidates could be considered for stereotactic ablative radiotherapy (SABR) or radiofrequency ablation. Primary Tumour Resectable Or Metastatic Disease After Resection of Primary Resectable or Potentially Resectable Metastatic Disease** Version 2013.5 Consider neoadjuvant therapy to convert to resectable Symptomatic treatment as appropriate. Chemoradiotherapy Palliative Resection of Primary Tumour In the presence of overt, serious symptoms, such as acute significant bleeding, obstruction, or unequivocal imminent risk of obstruction Diverting Ostomy Stenting Rectal Cancer Treatment Pathway Local Recurrence Version 2013.5 Page 7 of 7 Multidisciplinary Referrals to Create Individualized Care Plan Surgeon* Resectable From Colorectal Cancer Followup Care Pathway Locally Recurrent Disease MCC Evaluate for resectability MCC Guidelines and Resources Preoperative Chemoradiotherapy Consider even in the setting of previous pelvic radiotherapy Resection +/- Chemotherapy Radiation Oncologist Medical Oncologist Unresectable Palliative Care & Psychosocial Oncology Team *Opinion from a surgeon with relevant expertise should be obtained (e.g., Hepatobiliary or thoracic surgeon) NOTE: All patients under consideration for a temporary or permanent ostomy should be referred to an Enterostomal Therapy Nurse preoperatively. Patients should have access to an Enterostomal Therapy Nurse before and after ostomy surgery. NOTE: Once diagnosis is made, refer to early psychosocial oncology and palliative care team where appropriate Radiation Therapy Consider even in the setting of previous pelvic radiotherapy with or without Chemotherapy Appropriate Palliative Therapy Proceed to Colorectal Cancer Follow-up Care Pathway