Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cysticercosis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Hepatitis B wikipedia , lookup
West Nile fever wikipedia , lookup
Brucellosis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Whooping cough wikipedia , lookup
Leishmaniasis wikipedia , lookup
Meningococcal disease wikipedia , lookup
Marburg virus disease wikipedia , lookup
Orthohantavirus wikipedia , lookup
Yellow fever wikipedia , lookup
1793 Philadelphia yellow fever epidemic wikipedia , lookup
Typhoid fever wikipedia , lookup
Yellow fever in Buenos Aires wikipedia , lookup
Schistosomiasis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Leptospirosis wikipedia , lookup
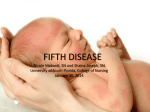
Paediatrics Topics Dr Shivani Pathmasrirengan GP ST2 Viral exanthems RASHES A Coxsackie virus B Measles C Parvovirus D Rubella E Toxoplasmosis F Varicella G CMV H HSV I Scarlet Fever Questions 1) 3 year old has generalised maculo-popular rash with conjunctivitis, rhinorrhoea, red lips + lesions on her inner cheeks. 2) 2 day old baby develops a vesicular rash. Her mother has had a recent febrile illness + crops of papules that are now forming blisters 3) An 18 month old child who has not been immunised develops a rash starting on her face which then spreads to rest of body. She is febrile with painful lymphadenopathy including suboccipital nodes. Measles (Rubeola) • Paramyxovirus • Incubation : 14 days • Preceded by Fever, cough/coryza, red eyes (conjunctivitis) • KOPLIK spots (white spots on buccal mucosa)- PATHOGNOMONIC!! • RASH- maculo-papular, face behind the ears- whole of body • Infective: prodromal sx – 4 days after onset of rash • Rx : SYMPTOMATIC • NOTIFIABLE illness !! Complications • Pneumonia • Otitis media • Febrile convulsions • Encephalitis – lethargy, headache , irritability • Sub-acute sclerosing pan-encephalitis (SSPE)- >7yrs after Measles inf Viral exanthems Rubella (German Measles/ 3-day measles) • Incubation : 16-18 days • Low grade- Fever, URTI sx, tender LYMPHADENOPATHY(post-auricular) • Appear less unwell than with measles ! • RASH- starts face/neck-then trunk - fades 3-5 days • Infective : 1 week before onset rash – until 4 days after • NOTIFIABLE disease!! Complications • Congenital Rubella – if infected in Pregnancy !! (if non-immune)1st tri • • • • • Cataracts Deafness Cardiac abnormalities Microcephaly/mental handicap IUGR • No effective Rx – Prevention by immunisation !! Viral exanthems Questions • 2 yr old girl presents with MILD FEVER + erythematous RASH on her cheeks, rash spreads to her trunk + persists for several days. What is the BEST advice? • 1) This is a very mild childhood illness in healthy children • 2) Avoid pregnant women, immunocompromised, and those with haematological conditions • 3) Exclude from nursery for 7 days after onset of rash • 4)Blood test is recommended to confirm diagnosis • 5) NONE of above Fifth Disease/ Erythema Infectiosum • Slapped Cheek Syndrome • Parvovirus B19 • Incubation: 4-14 days • Common winter + spring • Preceding occ low grade fever, sore throat, malaise, myalgia • RASH - slapped cheeks(red)- fades over 1-4 days , trunk lacy reticular pattern (usually biphasic - can recur for weeks to months afterwards with triggers such as sunlight, exercise, temperature change, bathing) • Not infectious once rash appears!! Complications • Advise : AVOID pregnant women , immunocompromised + haematological conditions ( sickle cell, thalassaemia) • Hydrops foetalis (severe anaemia)+ death – infected in pregnancy in 1st trimester! • Transient APLASTIC Crisis ! Viral exanthems Roseola (Exanthema subitum) • HHV 6/7 • Incubation: 9-10 days • Affects the young up to 3 yrs old • High fever 3 days settles as rash starts, abdo pain/malaise • Rash – first TRUNK, then arms, neck , v little on face/legs (L1-2days) • Common cause of FEBRILE convulsions !! • Mild self-limiting illness • Rarely : Encephalitis Viral exanthems Scarlet Fever • Streptococcus pyogenes • Incubation : 3-8 days • Fever, sore throat , headache • RASH – fine papular red rash – feels like “sand paper” Starts chest/stomach- entire body • “Strawberry tongue”, perioral pallor • As rash fades - peeling affects the fingertips, toes and groin area (desquamation) • NOTIFIABLE disease !! Complications • Pneumonia • Meningitis • Ear infection • Bone/joint problems • Renal /liver damage • Rheumatic Fever with assoc cardiac complications(AV/MV stenosis) • Rx : Penicillin 10 days Kawasaki Disease Fever >= 5 days + atleast 4 of: • B/L conjunctivitis (non-purulent) • Cervical Lymphadenopathy • Polymorphous rash • Mucous membrane: Strawberry tongue, pharyngeal inj, dry fissured lips • Changes in extremities: arthralgia, fingertip desquamation+ swelling hands/feet. Vasculitis : small-medium arteries- coronary artery aneurysms!! Rx: ASPIRIN + IV IMMUNOGLOBULIN Viral exanthems Hand, foot and Mouth Disease • Coxsackie A16, A10 and the echovirus • Incubation: 3-5 days • Painful ulcerative lesions – red macules/papules, yellow-grey ulcer mouth, oval pearly-grey vesicles hands + feet – no scarring • Highly infectious !! • Complications (rare): Viral meningitis, encephalitis. Viral exanthems Chicken Pox • Varicella Zoster virus • Incubation: 14-21 days • Fever, cold like sx ,myalgia • Crops of red flat macules which become raised(papules) then blister(vesicles- v itchy) and crust. • Lesions at different stages (Last 4-10 days) • Infectious : 1-2 days BEFORE rash appears till all lesions have CRUSTED over (commonly 5-6 days after onset of illness) • NOT a notifiable disease !! Complications • 2ndry bacterial skin infection-(eg impetigo, cellulitis, necrotizing fasciitis) (more common in eczema) • Pneumonia • Neuro : Encephalitis, Acute Cerebellar ataxia • Rarer: Myocarditis / Glomerulonephritis / pancreatitis/ HSP/arthritis Complications • ADULTS (more widespread rash/prolonged fever) : Severe CV/lung/ Smokers – fulminating varicella pneumonia • PREGNANCY: (mother) Severe chickenpox/ varicella pneumonia(2nd/3rdtri) • Fetus : risk of the Fetal/congenital varicella syndrome (1st 20-28 wks): • • • • • shortened limbs skin scarring Eye defects (cataracts, chorioretinitis) growth retardation Neuro: LD , microcephaly • LATER stages of pregnancy: PREMATURE delivery or neonatal chickenpox (esp serious if infected 7 days before birth+ 1week after delivery ) • Neonates: disseminated/haemorrhagic varicella Management • Sx Rx : paracetamol/ calamine lotion/piriton (itch) • ADVICE: encourage fluid intake/wear smooth, cotton fabrics/dress app to avoid overheating/shivering/ keep nails short • Avoid contact with pregnant/immunocompromised/neonates!! • Children should be kept away from school/nursery for 5 days from the onset of the rash. • Seek medical advice- if develop complications/ condition deteriorates! Management • Adult/ adolescent (>14yrs): presents within 24hrs of rash onset esp if smokers, on steroids: consider ACICLOVIR. Pregnant woman : Urgently Seek specialist advice: • Counselling risk of FVS • RCOG guidelines: 7 day course aciclovir (with informed consent) if presents within 24hrs of onset of rash + 20 wks preg or more !! • F/U (detailed US 5 wks after inf/at 16-20wks). Close monitoring. • ADMIT if has chest/neuro Sx/haemorrhagic rash/bleeding/severe eg dense rash + mucosal lesions) Management Breastfeeding Woman: • Consider ACICLOVIR- if presents within 24hrs of rash onset. • Seek specialist advice: • DoH: Baby: VZIG (if mother had lesions 7 days before/after delivery) or IV aciclovir • HPA : continue breast feeding, if lesions close to the nipple, milk should be expressed from affected side until lesions have crusted. expressed milk can be fed to the baby if he/she is covered by VZIG and/or aciclovir. Neonates: REFER: Rx aciclovir. Exposed to Chickenpox • Is the diagnosis of chickenpox in the contact is certain? • Was exposure SIGNIFICANT enough to put person at risk ? • Other Person has exposed zoster lesions, • Timing: Infectious period • Closeness of contact: maternal/neonatal contact, continuous home contact, in same room for 15 mins or more (eg house/classroom, 2-4 bed hosp bay) , face-face contact eg conversation • Has person had chickenpox in the past ? • ? Incr risk of complications: Pregnant /immunocompromised/neonate Exposure Pregnant woman : • If definite hx of chickenpox/shingles in past = IMMUNE: Reassure!! • If no hx/uncertain hx: Test for Varicella-zoster immunoglobulin (IgG) abs (in 1ry care if test results will be available in 2 days of exposure) otherwise seek specialist advice : test/ VZIG prophylaxis • Ab +ve = Immune : Reassure !! • Ab –ve: VZIG within 10 days of exposure !! • Protection is NOT absolute – contact doctor if develops rash!! Vaccinations 2 mo , 4 mo , 12-13 mo: Men B (2015) 2-8yrs: Nasal flu spray every yr (LAIV) Pre-school booster: 3, 4-5yrs 12-13yr GIRLS: HPV (2 doses) Selective Vaccines • Influenza (yrly)/pneumococcal >= 65yrs + high risk groups (asplenia, chronic resp /heart conditions, chronic neuro conditions(PD,MND,LD), diabetes, CKD, CLD, immunosuppressed) • BCG : parents/grandparents from high TB incidence grp • Hep B vaccine : Babies of Hep B inf mothers: birth, 1mo, 2 mo + 1 yr • Pregnant women : Flu vaccine, Pertussis from 20 wks gest • HIV +ve children: CI : BCG, yellow fever(MMR can be given) MMR = live vaccine • • • • MRC have NOT found any link between MMR vaccine + IBD or autism. SE: Fever , malaise, rash (1 week after, last 2-3/7), parotid swelling, ITP If in doubt about MMR status – MMR should be given !! Egg allergy/ anaphylactic reaction to egg is NOT a CI : under medical supervision • Confirmed anaphylactic rn to egg should NOT receive influenza/yellow fever vaccine • CI : pregnancy, neomycin and gelatin allergy, severe anaphylaxis to prev MMR , severe immunosupp • Can be given to HIV pts. Questions A child of 16 weeks is about to be immunised. Which one of the following would be a contraindication to vaccination? 1) Cystic fibrosis 2) Existing febrile illness 3) History of congenital heart disease 4) History of epilepsy in sibling 5) History of febrile convulsions Post-pone • Acute/current febrile illness • An evolving neurological condition (including poorly controlled epilepsy) • Administration of another live vaccine within three weeks of proposed MMR vaccination • Administration of immunoglobulins within three months of the proposed MMR vaccine. Questions • A sibling of an inpatient on a ward with severe immunosuppressed children visits and plays with the other patients. The following day she develops the 1st crop of chicken pox lesions. What is the BEST management? 1) Varicella Zoster immunoglobulin (VZIG) to the high-risk contacts 2 Immunise the child herself 3) Immunise the at-risk children 4) Oral aciclovir to the high-risk children 5) No immediate action needed; observe for signs in the high risk children • Thank you !! References • http://cks.nice.org.uk/chickenpox • Public Health England: Guidance on viral rash in pregnancy https://www.gov.uk/government/publications/viral-rash-in-pregnancy • http://www.nhs.uk/chq/Pages/can-i-have-vaccinations-if-impregnant.aspx?CategoryID=67 • https://www.gov.uk/government/uploads/system/uploads/attachment_da ta/file/532787/PHE_Complete_Immunisation_Schedule_SUMMER2016.pdf • http://www.pcds.org.uk/clinical-guidance/viral-exanthems