Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
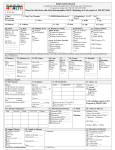
Module 14 – March 2010 Diagnosing and Treating Latent TB Infection (LTBI) Project Partners Funded by the Health Resources and Services Administration (HRSA) Module Overview Current methods for diagnosing TB infection Treatment options Monitoring Learning Objectives Upon completion of this session, participants will be able to: State the two methods for diagnosing TB infection Determine the groups that would most benefit from treatment for latent TB infection (LTBI) Determine LTBI treatment options and related monitoring Current Terms and Definitions Latent TB infection (LTBI) = presence of M. tb organisms without symptoms or radiographic evidence of TB disease Treatment of LTBI replaces “preventive therapy” and “chemoprophylaxis” Tuberculin Skin Test (TST) replaces PPD when referring to the Mantoux tuberculin skin test procedure or result Diagnosing LTBI Mantoux TB Skin Test (TST) Blood Assays for M. tb: QuantiFERON® Gold and In-Tube T-SPOT.TB ® Tuberculin Skin Test (TST) THEN NOW Standard Tuberculin Preparations Current preparations of tuberculin contain a purified protein derivative (PPD) of Koch’s Old Tuberculin The two standard preparations are: • USA: PPD-S – dose of 0.1 ml contains 5 tuberculin units (TU) of PPD • UK: PPD-RT-23 – dose of 0.1 ml contains 2 TU (equivalent to 5TU of PPD-S) Administering the TST Locate and clean site, stretch skin with thumb Inject 0.1 ml of 5 TU PPD-S intradermally at a 10°-15° angle, on volar surface of lower arm using a 27-gauge needle, bevel up Produce a wheal 6 - 10mm in diameter Do not massage injection site Reading the TST Record site, date and time of injection as well as PPD lot number Measure reaction in 48 to 72 hours Measure induration (palpable swelling), not erythema Forearm: Transversely to the long axis of the forearm. Record in mm! Ensure trained health care professional measures and interprets the TST TST Interpretation ≥ 5 mm ≥ 10 mm HIV-infection Other immunosuppressed Recent contact Fibrotic CXR changes Organ transplant recipients ≥ 15 mm Consider significant “positive” for all Recent immigrants Injection drug users Lab personnel Residents/employees of congregate settings Persons with clinical risk factors Children < 5-years-old or child/adolescent exposed to high-risk adult What factors might produce a false-positive TST result? False-Positive TST (2) Factors that may cause false-positive TST are: Non-tuberculous mycobacteria (NTM) BCG vaccination • Consider a positive TST result to indicate TB infection if risk factors are present BCG and TST Interpretation BCG is the most widely used vaccine in the world Wang, et al – meta-analysis • Effect of BCG vaccination on TST results was less after 15 years • Positive TST with indurations of >15 mm more likely to be result of TB infection than of BCG vaccination L Wang, et al. Thorax 2002;57:804-809 What factors might produce a false-negative TST result? False-Negative TST (2) Factors that may affect the ability to respond to the TST include: Anergy (the inability to react to a TST because of a weakened immune system) Recent TB infection (up to 8-10 weeks following exposure) or infection many years ago Recent live-virus vaccination/infection (e.g., measles) Overwhelming TB disease Very young age (newborns < 6 months old) Poor administration technique (e.g., TST placed too shallow or too deep) Blood Assays for M. tuberculosis QuantiFERON®-TB Gold In-Tube (Cellestis Ltd, Victoria, Australia) • Measures Interferon-gamma (IFN-y) T-SPOT.TB (Oxford Immunotec Ltd, Oxford, UK) • Measures peripheral blood mononuclear cells that produce IFN-γ Blood Assays for M. tuberculosis (2) There is limited data on how these tests perform in certain populations: • Children (≤ 5yrs) • Recent contacts Cost and access to these tests may be two of the greatest barriers to use in the Caribbean Clinical Pearl-Testing Negative TST or Blood Assay for M. tuberculosis does not exclude TB disease! Rule Out Active TB Before initiating single-drug treatment (monotherapy) for LTBI, active TB disease must be ruled out with: • Chest X-ray • Clinical evaluation Treating Latent TB Infection LTBI Treatment: Isoniazid (1) INH remains the mainstay of LTBI treatment Duration of treatment? • HIV-infected or radiographic evidence of prior TB: 9 months preferred 6 months acceptable • All others 6 months Completion of Treatment Completion of therapy is based on total number of doses administered, not on duration alone! Count doses, not months • 9 mo INH daily — 270 doses within 12 mo • 6 mo INH daily — 180 doses within 9 mo • 4 mo RIF daily — 120 doses within 6 mo Interruption of more than 2 mo — medical evaluation to rule out active TB before restart Isoniazid: Hepatitis Incidence of hepatitis in persons taking INH is lower than previously thought (0.1 to 0.15%) Hepatitis risk increases with age • Uncommon in persons <20 years old • Nearly 2% in persons 50 to 64-years-old Risk increased with underlying liver disease or heavy alcohol consumption Monitoring During Treatment Baseline laboratory testing should be obtained for patients starting INH when: • HIV infected • Pregnant or immediate postpartum (within 3 months) • History of chronic liver disease or heavy alcohol use • Initial evaluation suggests a liver disorder Evaluate monthly for: • Adherence • Symptoms (particularly for hepatitis) Supplemental Pyridoxine (B6) Peripheral neuropathy occurs in < 0.2 % using conventional Isoniazid (INH) doses Add vitamin B6 (pyridoxine) supplement (25-50mg daily) for patients with: • Diabetes, HIV, renal failure, alcoholism, malnutrition, advanced age • Pregnant or breastfeeding mothers (and infant) • Patients with a seizure disorder Patient Education Patients should be instructed to stop medication and seek immediate medical consultation if they experience loss of appetite, abdominal pain, nausea, vomiting, jaundice or other symptoms of hepatitis. Monthly face-to-face interview Rationale for treatment Adherence Symptoms of adverse drug effects Plans to continue treatment Withholding Isoniazid INH should be withheld when: Transaminase levels exceed • 3 times the upper limit of normal if associated with symptoms; or • 5 times the upper limit of normal if the patient is asymptomatic Treating Latent TB Infection Special Situations LTBI Treatment: INH Resistant Contacts of INH-resistant TB: • 4-6 months of rifampicin (longer for children and immunocompromised) daily • Consider use of rifabutin in HIV-infected patients on rifampicin-incompatible protease inhibitors For persons intolerant of INH, use 4 months of rifampicin daily • 6 months RIF for children and persons with HIV infection LTBI Treatment: Pregnancy Treatment for LTBI during pregnancy is controversial • Wait until after delivery? • Possible increase hepatotoxicity during pregnancy and early post-partum Treatment for LTBI with close clinical and laboratory monitoring should be encouraged if the woman is also: • HIV-infected or • a close contact to an infectious TB patient LTBI Treatment: Breastfeeding Breastfeeding is not a contraindication • Infant will get a small amount of INH (sub-therapeutic) • No toxic effects reported Give both mother and infant vitamin B6 (pyridoxine) LTBI Treatment: MDR-TB No drug regimens with proven efficacy for LTBI resulting from exposure to MDR-TB Treatment may be indicated in some highrisk situations (seek consultation with an MDR-TB expert) Clinical follow-up recommended for 2 years post-contact Window Period Prophylaxis Window period – refers to the interval between infection and detectable reactivity to the TST Treatment during the window period: • should be considered for children < 5 and persons with significant immunosuppression • can be discontinued if, after 8 weeks, a repeat TST is negative and child remains asymptomatic Contacts with HIV or severe immunosuppression should complete the full course of treatment regardless of repeat TST Re-treatment of LTBI Real issue is the probability of acquiring new infection Recommended for those who have HIV infection and children who have been in contact with a sputum smear-positive case Counseling A Patient With LTBI NEVER say: You’ve been “exposed” so you need to be treated. INSTEAD say: You have been exposed and infected with the TB germ. But don’t worry… Good news: You do not have the disease and you are not contagious to anyone Bad news: It is sleeping in your body, can wake up later, make you very ill and contagious to others Counseling A Patient With LTBI (2) Why get treated? Treatment will prevent future disease and protect you and those close to you. Warning: Taking medication for 6-9 months is a long time but it takes that long to kill all or most of the TB germs “TOUGH bugs”… so take your medicine correctly and completely! Treatment of LTBI: Summary Assess for TB risk factors If risk is present, perform test for TB infection (TST or blood assay for M.tb) If test for TB infection is positive, rule out TB disease If TB disease is ruled out, initiate treatment for LTBI If treatment is initiated, monitor patient regularly and ensure completion!