Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
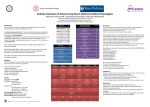
Adverse Drug Events – What Do We Really Mean? Definitions: Adverse Drug Event (ADE): Injury resulting from medical intervention related to a drug (IOM). Adverse Drug Reaction (ADR): Any response to a drug which is noxious and unintended which occurs at doses normally used in man for prophylaxis, diagnosis, or therapy of disease, or for the modifications of physiological function1 (Figure 1). Relationship between ADE & Medication Errors An Adverse Drug Event (ADE) is harm associated with any dose of a drug, whether the dose is “normally used in man” or not. An Adverse Drug Reaction (ADR) is a subtype of an ADE (i.e., all ADRs are ADEs, but not vice versa) and by definition, drug-induced harm occurring with appropriate use of medication (i.e., not caused by an error). While ADEs are medication-related patient injury events, medication errors encompass all errors that may occur at any stage of the medication process, with or without patient harm (Figure 2). Some ADEs arise as a result of an error and are considered preventable. Others arise from ADRs, where the medication is used in a proper manner and are considered non-preventable ADEs. Potential ADEs (pADEs) are incidents where patient harm could have occurred, but did not either because of chance or intervention.2 Adverse Drug Event (ADE): Preventable vs. Non-preventable Patient Harm Preventable Harm 1 2 Medication Error that reached patient Source: World Health Organization (WHO) Source: Pediatric Drugs. 2009; 11:153-160. Non-Preventable Harm Adverse Drug Reaction (ADR) Allergy Relationship between Medication Errors and Preventable ADEs (pADEs) A medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient or consumer. Such events may be related to professional practice, health care products, procedures and systems – including: prescribing, order communication, product labeling, packaging and nomenclature, compounding, dispensing, distribution, administration, education, monitoring and use. pADEs occurs due to medication errors or mishaps (several definitions state that pADEs are also known as “near misses” or “close calls”). pADEs are identified medication-related problems (MRPs)/drug-related problems (DRPs)/ medication-therapy problems, these may include, but are not limited to, medication errors. Drug Therapy Problem Categories Appropriateness More effective drug available pADE On unnecessary drug therapy pADE Does the patient have an indication for a medication that is not being treated or prevented? Needs additional drug therapy pADE Lab monitoring needed for screening pADE Is the most effective drug product being used for the medical condition? Needs different drug pADE Lab monitoring needed efficacy pADE Dose too low pADE Lab monitoring needed for safety pADE Undesirable effect ADE Contraindication pADE Drug interaction ADE or pADE Is the dose appropriate and able to achieve the intended goals of therapy? Is the patient experiencing an adverse event from the medication? Is the dose so high it could cause toxicity in the patient? Adherence ADE/pADE Is the medication appropriate for the medical condition being treated? Effectiveness Safety Drug Therapy Problems Is the patient able to take the medication as intended? Dose too high pADE Cannot afford pADE Forgets to take pADE Directions not understood pADE Unable to administer correctly pADE Patient Case Examples pf pADE and ADE Patient Story: MS is a 52-year-old female admitted to the hospital for pneumonia. Her past medical history includes depression, high cholesterol and high blood pressure. Her medications include Fluoxetine 20mg, Atorvastatin 40mg, lisinopril 20mg and warfarin 2.5mg. Upon interviewing the patient, the pharmacist reveals that MS had had a TKN 5 months ago and that’s when she started taking warfarin. Following assessment of the patient specific information and the rest of the medication history, the pharmacist identifies a medication related problem. Why is this story a Medication Error? Following a TKR warfarin or other anticoagulant should be continued for 14 days per ACCP Chest guidelines Questions: What is the medication related problem (pADE)? What kind of medication error is this? • • • • On unnecessary drug therapy Error in prescribing, communication and monitoring Answers: Patient Story: KW is a 65-year-old male with history of diabetes, dyslipidemia and a recent hospitalization where he was treated for a pulmonary embolism. Upon discharge, KW was given a new prescription for warfarin 2mg daily, information for ADR self-monitoring as well as information for a follow up appointment with his PCP. After several doctor visits, KW’s INR is stabilized at 2.4 (goal 2-3) and since he does not report having any issues, his weekly appointments get extended to monthly visits. Three months later, KW is hospitalized for complaints of dizziness, lethargy and shortness of breath. Upon further examination, his labs revealed a therapeutic INR of 2.6 and a low H&H of 7g/dl and 22% respectively. KW reports proper adherence to his medications and denies any injury leading to bleeding. A stool guaiac test is performed and comes back positive. Questions: What kind of medication-related patient harm is this? Answers: • Non-preventable; ADR • Patient Story: PR is a 78-year-old female nursing home resident with history of high blood pressure. PR started complaining of pain in her lower back from an injury she sustained in the past. She describes her pain as sharp stabs and rates it as a 9 in a 0-10 scale. PR denies any previous history of opioid use having controlled her sporadic pain with Tylenol and Advil. Unfortunately her pain is now uncontrollable and her doctor prescribes Fentanyl patch 12.5 mg. One week after the new pain medication was started, the nursing home staff notices difficulty swallowing and increased altered mental status. Why is this story a Medication Error? Initiating the use of long-acting opioids (LAOs) in opioid-naïve individuals (those who have never taken opioids) has been highlighted by the U.S. Food and Drug Administration (FDA) as a potentially dangerous practice Questions: What kind of medication-related patient harm is this? What kind of medication error is this? • • On unnecessary drug therapy Error in prescribing and monitoring Answers: • • Patient Story: JM is a 66-year-old female who was recently discharged home after a long stay in ICU and subsequent rehab. Her medication list prior to admission included amiodarone 200mg daily atorvastatin 40mg daily, Lisinopril 10mg daily and glyburide 5mg twice daily. Upon admission to ICU her glyburide was discontinued and intensive insulin therapy was started. She was subsequently discharged on insulin sliding scale. It has now been a few months since her rehab stay and JM presents to her doctor’s office with complaints of dizziness, clamminess and an episode of fainting which did not result in a fall. Upon review of the medication list, it is found that JM continued to take her glyburide 5mg twice daily in conjunction with her newly prescribed insulin. Why is this story a Medication Error? Hyperglycemia frequently occurs with acute medical illness, especially among patients with cardiovascular disease. This has been linked to increased morbidity and mortality in critically ill patients. An expanding body of literature describes the benefits of normalizing hyperglycemia with insulin therapy in hospitalized patients Questions: What kind of medication-related patient harm is this? What kind of medication error is this? • • • • On unnecessary drug therapy Error in communication Answers: This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (NE QIN-QIO), the Medicare Quality Improvement Organization for New England, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. CMSQIN_C3-2_201508_0174