Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropharmacology wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Drug interaction wikipedia , lookup
Plateau principle wikipedia , lookup
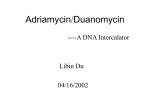
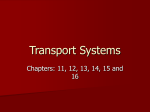
[CANCER RESEARCH 43, 3417-3421, July 1983] Plasma Pharmacokinetics of Adriamycin and Adriamycinol: Implications for the Design of in Vitro Experiments and Treatment Protocols Raymond F. Greene, Jerry M. Collins,1 Jean F. Jenkins, James L. Speyer, and Charles E. Myers Clinical Pharmacology Branch [R. F. G., J. M. C., J. F. J., J. L. S., C. E. M.], National Cancer Institute, and BiomédicalEngineering and Instrumentation Branch [J. M. C.], Division of Ftesearch Services, NIH, Bethesda, Maryland 20205 ABSTRACT tion (25). A physiological model of Adriamycin pharmacokinetics based solely on flow limitation for tissue uptake and first-order The plasma pharmacokinetics of Adriamycin and adriamycinol following a 15-min infusion of 75 mg/sq m of Adriamycin were studied in ten patients previously untreated with Adriamycin. The disappearance kinetics of Adriamycin could adequately be de scribed by a biexponential equation with an initial half-life of 8min and a terminal half-life of 30 hr. The major drug exposure (area under the concentration-time curve) occurs during the terminal phase where drug concentrations are generally less than 10"7 M (0.05 ng/m\). An improvement in the high-perform elimination by the liver has simulated the actual experimental data in rabbits and humans reasonably well (9, 17). Compart- ance liquid chromatography sensitivity facilitated the determina tion of the terminal phase. The plasma kinetics of adriamycinol, the major and only known active metabolite of Adriamycin, show a rapid initial increase in plasma concentration followed by a slow decline which parallels that of Adriamycin during the termi nal phase. The relative drug exposure of adriamycinol to Adria mycin was approximately 50%. The relationship between the measured plasma drug levels and free drug available for distribution into tissues was studied by comparing the plasma binding characteristics of Adriamycin and adriamycinol. A constant 20 to 25% of the total plasma concentrations of both Adriamycin and adriamycinol was freely diffusible over the whole range of observed concentrations, 20 nw to 2 MM. Thus, the free drug exposure (area under the concentration-time curve) of tumor and host tissues in vivo can be determined from these plasma measurements, since the free drug exposures in plasma and in extracellular fluid are equivalent. These results can also serve as a guide for the design of clinically relevant in vitro studies of Adriamycin and adriamycinol. The pharmacokinetic parameters determined in this study have been used to simulate plasma concentration-time courses for a variety of Adriamycin treatment schedules. Alternatives are sug gested which reduce peak plasma Adriamycin concentration while antitumor area under the concentration-time curve is main tained. INTRODUCTION Adriamycin is an antitumor agent used in the standard chem otherapy regimen of most hematological and many solid tumors (8). Adriamycin is commonly administered clinically as a bolus dose of 60 to 90 mg/sq m every 3 weeks (7). The plasma kinetics of the drug following bolus administration exhibit a rapid initial decline followed by a slow decline in plasma concentration which has been ascribed to the ability of tissues to rapidly accumulate the drug intracellularly followed by a slow release of the drug from tissue stores as plasma levels decline due to drug elimina 1To whom requests for reprints should be addressed, at Building 10, Room 6N119, NIH, Bethesda, Md. 20205. Received October 7, 1982; accepted April 11, 1983. JULY 1983 mental modeling has also been used to describe the disposition of Adriamycin in plasma. Initially, a biphasic loss of the drug was proposed based on total fluorescence or radioactivity assay methods (5, 12). The use of assay methods specific for Adria mycin led to the inclusion of an intermediate phase showing a triphasic loss of the drug (4, 6, 24), although no compelling pharmacokinetic or pharmacodynamic justification for the third phase has been proposed. Although many studies of the plasma pharmacokinetics of Adriamycin have been undertaken, certain deficiencies make the interpretation of the pharmacokinetic data or its relevance to the clinical use of Adriamycin difficult to understand: (a) The plasma kinetics of Adriamycin have been fairly well studied for time periods of up to 24 hr following a bolus injection; however, the terminal half-life of Adriamycin is about 30 hr, which requires sampling for several days for adequate characterization, (b) Metabolism of Adriamycin requires assay techniques which sep arate parent drug and metabolites and allow sensitive quantitation of Adriamycin and other metabolites of interest. The pres ence of active metabolites can obscure the evaluation of either the therapy or toxicity of the drug unless the activity of the metabolite is evaluated. This general difficulty has been com pounded in the case of Adriamycin, since much of the original metabolite data was subsequently ascribed to artifacts from the analytical methodology (23). (c) Although it is thought that only free drug is available to produce drug effects, prior studies have not quantitated the binding of either Adriamycin or adriamycinol over the range of observed concentrations. The primary purpose of this study is to provide a complete description of the plasma pharmacokinetics of Adriamycin and adriamycinol. The relevance of the pharmacokinetic parameters to the in vivo and in vitro efficacy and toxicity of the drug is discussed. Pharmacokinetic and pharmacodynamic principles are applied to practical issues of Adriamycin scheduling and cardiotoxicity. MATERIALS AND METHODS Clinical Characteristics. Ten patients undergoing single-agent Adri amycin therapy for metastatic breast cancer, metastatic soft-tissue sar coma, or nodular lymphomas, who had not been treated previously with Adriamycin, were studied during their first course of Adriamycin therapy. Adriamycin was administered at a dose of 75 mg/sq m through a fresh i.v. infusion line over 15 min. As part of a study on cardioprotection, 2 The abbreviations used are: NAC, N-acetyl-L-cystelne; HPLC, high-perform ance liquid chromatography; C x / or AUC, area under the concentration-time curve. 3417 Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1983 American Association for Cancer Research. R. F. Greene et al. some patients were randomly selected to receive 5.6 g/sq m of MAC2 from: p.o. 1 hr before the dose of Adriamycin. All 10 patients had prior surgical resections, but only one patient had prior chemotherapy (with strepto- % of drug bound zotocin). Liver function tests were within the normal range for all patients at the time of study. Sample Analysis. Blood samples were obtained at 0-, 0.08-, 0.17-, 0.5-, 1-, 3-, 6-, and then 24-hr increments following administration of the drug for at least 3 days. Blood samples were generally collected from a vein on the opposite arm from the infusion. If necessary, samples were taken from the same vein used for infusion, after extensive flushing. No major differences were observed between patients sampled by the 2 methods. The most likely error would be an overestimate in the early samples. Since most of the drug exposure is in the later phases, such an error would not be critical. The blood was collected in glass tubes containing EDTA and were immediately placed on ice to prevent metabolism by the cellular blood components. The blood was centrifugea at 600 x g for 10 min to obtain plasma which was frozen at -40° until analyzed. Each plasma sample was analyzed for Adriamycin and adriamycinol by means of a HPLC with fluorescent detection capable of separating and yielding sensitive and specific quantitation of each compound. Sam ples were prepared for analysis by adding 1 ml of 0.1 M sodium borate buffer (pH 9.8) and 50 ng daunomycin as an internal standard to 1 ml of the plasma sample and extracting the drug into 17 ml of chloroforrrrmethanol (4:1, v/v) in a 50-ml glass tube. The organic layer was transferred to a conical glass tube and evaporated to dryness under nitrogen at room temperature. The residue was redissolved in 150 ^l methanol, and an aliquot was injected into the HPLC. Exposure of the samples to light was limited as much as possible. Standards containing Adriamycin (0 to 200 ng/ml), adriamycinol, and Adriamycin aglycone in plasma were processed in an identical fashion and used for quantitation. The HPLC system used was essentially the reverse-phase system described by Israel et al. (18) with one modification. An excitation wavelength of 228 nm rather than 482 nm was used which yielded an approximately 10-fold increase in sensitivity for each compound. No evidence of interfering fluorescent peaks was observed in "pre-" dose samples. Quantitation of drug concentrations was achieved by measuring the peak height ratios of drug:internal standard for the plasma standards and obtaining a least-squares fit of peak height versus concentration. The concentrations of Adriamycin and adriamycinol in the plasma sam ples were then obtained from the peak height ratios of the samples. The recovery of Adriamycin, adriamycinol, and the internal standard in the assay procedure was approximately 70% within the concentration range of the standards. The detection limit of the assay (signal of 5 times the average noise) was experimentally determined to be 2 nw for Adria mycin and adriamycinol using 1 ml of plasma. The within-day precision (C.V.) of the assay (n = 5) at 1 pM was 7.1% for Adriamycin and 8.2% for adriamycinol; at 10 nw, it was 11.2% for Adriamycin and 18.6% for' adriamycinol. Plasma Binding of Adriamycin and Adriamycinol. Plasma was used immediately after it was obtained from either normal volunteers or patients on this pharmacokinetic study, before or after treatment with NAC and/or Adriamycin. Plasma (1.2 ml) was spiked with Adriamycin and adriamycinol and added to one side of a commercial dialysis cell (Technilab Instruments, Pequannock, N. J.). An equal volume of phos phate or 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid buffer (0.1 M. pH 7.4) was added to the other side. Dialysis was performed at 37° in the dark, with gentle shaking. Preliminary studies showed that equilib rium was achieved between 12 and 20 hr and that the equilibrium pH was 7.4 in both plasma and buffer. The HPLC assay was used to determine the concentrations of Adriamycin and Adriamycinol in the plasma and buffer. [uC]Adriamycin was also used for binding experi ments after prepurification by HPLC. No decomposition of Adriamycin or adriamycinol was evident when dialysis times of less than 20 hr were used. The percentage of drug bound to plasma proteins was calculated 3418 (Plasma concentration —buffer concentration) Plasma concentration Pharmacokinetic Analysis. The Adriamycin plasma concentration-time data were fitted to a biexponential equation: Cp(f) = A exp(-«f) + B exp(-/fl) (B) where Cp(f) is the drug concentration at time, f, after an i.v. dose of the drug. A and B are constants, and «and ßare the apparent first-order elimination rate constants. The data fits were performed on MLAB, a nonlinear fitting program, using a 1/concentration squared weighting function (20). The areas under the curve (C x f ) of the initial and terminal phases for Adriamycin were calculated from the ratios of A/a and B/ß. The total AUC for Adriamycin and adriamycinol were also calculated based on the trapezoidal rule from zero to the last measured time point and then by first-order extrapolation to infinite time using the experimen tally determined half-life value for Adriamycin. The extrapolation averaged 14% of the total area for Adriamycin and 20% for adriamycinol. The percentage of drug exposure of adriamycinol in relation to Adriamycin was calculated from the ratio of the total AUC of adriamycinol to AUC of Adriamycin. The volume of distribution (V„)and total body clearance (ClrB) for Adriamycin were calculated by means of noncompartmental techniques: Dose (C) AUC Steady-state VK = (Dose) (AUMC) AUC2 (D) where the area under the moment curve (AUMC) was calculated using a published method (3). RESULTS Pharmacological Studies. Following the 15-min infusion of Adriamycin, the Adriamycin plasma concentration exhibited an initial rapid decline from approximately 5 to 0.1 ^M within 1 hr. This initial phase was followed by a slower decrease ¡nconcen tration which was fairly log-linear beyond 6 hr (Chart 1). A rapid IUWV1000/— (¿)_ Adriamycin 2Adriamycinol (O)\ (n=10)^M\ATe< 2 SZ Mean ±SD C •^rf'o 10°"5C"e " "~T - - ^f~~~^"^^~-2J_ o 10o 0 _L <bo 1AJ p iiii0 24 96TIME48 (hours) 72 Chart 1. Measured Adriamycin and adriamycinol plasma concentration-time terns following a 15-min infusion of Adriamycin 75 mg/sq m to 10 patients. CANCER RESEARCH pat VOL. 43 Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1983 American Association for Cancer Research. Clinical Pharmacokinetics of Adriamycin Table 1 Pharmacokinetic parameters obtained from biexponential analysis of Adriamycin plasma concentration-time Initial phase A (MM) Adriamycin alone* (n = 5) 3880 ±1078* Adriamycin + NAC (n = 5) 4970 ±2236 tin (min) 10.0 ±2.2 6.9 ±1.1 profile Terminal phase Cxi (nM-hr) B (nu) 933(21.7%) 77.2 ±10.5 f,/2 (hr) C x t (nw-hr) 30.2 ±1.9 3364(78.3%) 830(19.5%) 24.6 ±2.7 96.8 ±11.1 3436(80.5%) Combined groups (n = 10) 4425 ± 678 8.5 ±1.3 882(20.6%) 87.0 ± 7.9 27.4 + 1.8 3400(79%) 8 There was no significant difference (p > 0.2) in any parameter between groups given Adriamycin alone or Adriamycin plus NAC. 6« Mean ±S.E. increase ¡nadriamycin plasma concentration was observed in the first hr followed by a decline in concentration which generally paralleled that of Adriamycin. At the retention time for Adriamycin aglycone, only small fluorescent peaks were observed corre sponding to concentrations of generally less than 10 nw (based on the aglycone standard). The concentration-time data for Adriamycin for each patient were analyzed separately as described in "Materials and Meth ods" to obtain estimates of the pharmacokinetic parameters. Table 1 shows the relative contribution of each phase to the total AUC (C x f) and the estimates obtained for Adriamycin when the data were grouped by treatment category (Adriamycin alone versus Adriamycin plus NAC). No significant differences in the values of each group were evident. Using the data from all the patients studied, the pharmacokinetics of Adriamycin could best be fit to a biexponential equation of the form: Table 2 Noncompartmental values for the clearance (Cira) and steady-state distribution volume (V„) of Adriamycin and plasma drug exposure (C x T) of Adriamycin and Adriamycinol Adriamycin alone jg (mi/min/ sqm) 514 ±56C Adriamycin + MAC* 494 + 50 Adriamycin C x f* Adriamycinol C x fa V«(liter/kg) 28.0 ±3.3 (nM-hr) 4427 ±418 (nu-hr) 2137 ±472 22.4 ±4.4 4516 + 413 2422 + 565 504 + 35 25.2 ±2.7 4477 ±277 2280 + 350 Combined groups a Total drug plasma C x t. For both Adriamycin and Adriamycinol, multiply total by 0.25 to obtain free drug Cxi. 6 There was no significant difference (p > 0.2) in any parameter between groups given Adriamycin alone or Adriamycin plus NAC. c Mean ±S.D. drug exposure is directly proportional to the total drug exposure in plasma; and (c) the free drug exposure of adriamycinol is approximately one-half of that for Adriamycin. Cf(t) = 4147 exfX-5.39 f) + 82 exp(-0.0229 f) A biexponential model for Adriamycin appears to be sufficient where Cp(t) is the nw Adriamycin concentration, and time, f, is ¡n to describe the major features of both the pharmacokinetic profile and the pharmacological activity of Adriamycin. The initial phase hr. Table 2 shows the total body clearance and steady-state consists of a very rapid decline in plasma Adriamycin concentra tions. Initial concentrations are 50-fold higher than those ob volume of distribution of Adriamycin and the AUC of adriamycinol and Adriamycin for the 2 groups. Similar values were obtained; served at the start of the terminal phase. Despite the relative magnitude of the concentrations observed during the initial thus, the plasma pharmacokinetics of Adriamycin and adriamy cinol appear to be unaffected by administration of NAC. The Vss phase, the terminal phase provides 75% of the total drug expo of 25 liters/kg compares favorably with the tissue: plasma parti sure and maintains cytotoxic concentrations for several days, tion coefficients determined in a rabbit study (17). since the fi/2 is 30 hr. The biphasic curve can be used to examine Binding Studies. For nonradioactive drug (n = 12), Adriamycin the 2 patterns of Adriamycin therapeutic and toxic effects which was 74 ±1.7% (S.D.) bound, and adriamycinol was 76 ±1.4% have been observed: those due to high peak concentrations, bound. The percentage bound was independent of plasma con and those related to total drug exposure. centration over the range observed in this study, 20 nM to 2 U.M. In addition to its own pharmacological activity, Adriamycin is also metabolized to one known active metabolite, adriamycinol. There was no difference in Adriamycin binding for plasma sam The plasma kinetics of both compounds were determined in an ples from patients receiving NAC versus patients not receiving attempt to determine the relative importance of these 2 chemical NAC. At 1 (¿M, the [14C]adriamycin was found to be 82 ±0.7% species to the pharmacological activity observed after Adriamy bound by radioactivity measurements and 75 ±2.7% bound by cin administration. These studies showed a relative drug expo sure for total plasma adriamycinol of approximately one-half of the HPLC method. More than 95% of the total radioactivity initially present was recoverable in the plasma and buffer solu the value for total Adriamycin. Since equivalent plasma binding was found for Adriamycin and adriamycinol, the free drug expo tions at equilibrium. For both radioactive and nonradioactive studies, binding of the drug to the dialysis apparatus was cor sure ratio is the same as for total drug exposure. Studies of the rected for by sampling both the plasma and buffer sides of the relative cytotoxicity of Adriamycin and adriamycinol have shown dialysis membrane. that adriamycinol is less active than Adriamycin (22), at least for 1-hr exposures. Presumably, these short-term results are also applicable to longer exposures since, as discussed below, cy DISCUSSION totoxicity of Adriamycin is not directly time dependent (16). Thus, for patients with normal hepatic function, Adriamycin appears to The major conclusions drawn from the analysis of the phar be the principal species responsible for therapeutic effect. The macokinetic data for Adriamycin are: (a) the bulk of the drug role of adriamycinol may be more important in patients with liver exposure (C x T) occurs during the terminal phase: (b) the free JULY 1983 3419 Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1983 American Association for Cancer Research. R. F. Greene et al. :,A>Jli; do«9 lor 7S mo/m2 total Slmulollon. B InluilonSlnota Doy Conltnuou. for 75 mfl/m teto! dOM 5-t>oy Coflttnuoua Infutlon 2-Hour Ion— 1000 15 Ulnut. Int u. Slngi* Infuclon q?4*i x S 15-M1fiut« Infuilon 1000: \•? \; Chart 2. Simulated Adriamycin concentra tion-time patterns for a total dose of 75 mg/sq m administered by various schedules. A, shortterm (0 to 5 hr) patterns; B, long-term (up to 120 hr) patterns. q24h x 5, every 24 hr for 5 days. ; _1 P \ \ \ \ -X-.\\V, 100 C o 'S IDO "c \<KSimulation«3 o e o O u 10 k sÃ- 10 1234 24 TIME (hours) disease, since it has been reported that total adriamycinol plasma concentrations are higher than total Adriamycin plasma concen trations (10). Also, the importance of daunomycinol in the ther apeutic efficacy of daunomycin may be substantially different, since daunomycin is metabolized to the alcohol metabolite to a much greater extent resulting in daunomycinol plasma exposure much greater than that of daunomycin (2). The major purpose of this study has been to obtain an accurate and complete concentration-time profile of free Adriamycin and adriamycinol in plasma. Since the plasma binding of both Adria mycin and adriamycinol is constant over the observed range of plasma concentrations, the free drug concentration-time profile represents 20 to 25% of the total drug profile of Chart 1. The pharmacological activity of a drug is generally determined by the free drug. These plasma free-drug exposure measurements are directly applicable to both tumor and host tissue free-drug ex posure in vivo, i.e., for tissues which do not have substantial clearance of the drug, normal and tumor cells will be exposed to extracellular free-drug concentrations that are identical to plasma free-drug exposure. The design of in vitro experiments should also be guided by these principles. Since cells in vitro are exposed to drug via a medium which substitutes for extracellular fluid, it should be possible to evaluate the pharmacodynamic activity of Adriamycin in vitro under conditions which would yield the same free-drug exposure observed in vivo. None of the in vitro cell survival studies to date has considered the activity of the anticancer drug in relation to its free-drug concentration. These studies have included fetal calf serum in varying amounts in the incubation medium. The binding characteristics of Adriamycin in these prep arations are not known but should be investigated if the ultimate purpose for such studies is to make comparisons with clinically achievable exposures. Such an approach may provide better predictive capabilities than does the present standard method, which routinely uses an exposure of one-tenth of the peak total plasma concentration for 1 hr (1). There is a log-linear relationship for Adriamycin between the surviving fraction of tumor cells and concentration or exposure duration within the therapeutic range (13, 14). This relationship is typical of phase nonspecific agents (19): log S, = -k(C x f) where S, is the surviving cell fraction (A//A/0),and k is a propor tionality constant relating the C x T pattern to cell survival. The correlation of survival fraction with both concentration and time 48 72 96 120 TIME (hours) for Adriamycin has recently been studied under conditions rele vant to Adriamycin pharmacology (16). Exposure of human colon tumor cells to Adriamycin concentrations of 10, 100, and 1000 nM for either 2 or 24 hr demonstrated a good correlation between the C x T value and the log of the surviving fraction. The observed correlation of in vitro tumor cell survival and C x T suggests that the antitumor effects of Adriamycin are dose dependent, but schedule independent. Clinical studies of the antitumor effects of Adriamycin have supported this conclusion. It has been reported that Adriamycin is equally effective regard less of the administration schedule used, namely, weekly or triweekly bolus or continuous infusion (11,21 ). The importance of dose and schedule should also be viewed from the perspective of limitations imposed by host tissue toxicity. Both cardiotoxicity and drug-induced emesis have been reported to be schedule-dependent and may be more associated with the peak drug concentrations than with total drug exposure. These latter side effects have been lessened by an infusion rather than as a bolus, without any concomitant changes in the tumor efficacy or bone marrow depression (21 ). Earlier studies (8) suggest that bone marrow depression may be schedule dependent. Even this limited information about Adriamycin pharmacodynamics can permit the more effective use of pharmacokinetics towards a goal of optimal chemotherapy. Although the 2- to 5day continuous infusion schedule may be superior to bolus administration with respect to cardiotoxicity, it possesses draw backs in terms of practical implementation, especially in the setting of a large outpatient practice. The need for central venous catheter placement, a pump, and additional patient monitoring would make routine use of these protocols difficult. One practical application of pharmacokinetics is to predict concentration-time profiles for alternate dosing strategies. Using the pharmacokinetic data from Table 1 and standard formulas for schedule adjustment (15), we have explored a variety of delivery options and summarized the results in Chart 2. Dividing a single large dose into several smaller doses is one method of reducing peak concentrations. For example, the peak plasma Adriamycin concentration can be reduced 5-fold by simply split ting the single 75 mg/sq m dose into 5 daily doses of 15 mg/sq m. Lengthening the infusion time also lowers the peak plasma concentration. The peak concentration observed after a 15-min infusion, such as that used in this study, is already 40% lower than the peak concentration predicted for a 15-sec rapid i.v. 3420 Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1983 American Association for Cancer Research. Clinical Pharmacokinetics of Adriamydn push. An additional 6-fold reduction in peak concentration can be achieved by lengthening the infusion time from 15 min to 2 hr, which could still be administered peripherally. The combina tion of dividing the single dose into 5 daily doses and prolonging each infusion from 15 to 120 min provides an alternate schedule which produces a peak concentration 30-fold lower than that observed in the current study. No simple combination of divided doses and constant infusions actually produces a constant plasma concentration. For the alternate schedule, there is some daily increase and decrease in concentration, while the continuous infusion protocol only reaches steady state by the end of a 120-hr period. Both the intermittent 2-hr schedule and the 120-hr continuous infusion schedule provide comparable concentrations for most of the 5day period. For a 48-hr infusion, which has also been tested (21), the simulated plasma concentration rises throughout the infusion period. This behavior is expected for a drug with a controlling f1/2 of 30 hr. Whether this alternate schedule can reduce the incidence of cardiotoxic side effects to a level achievable by 2to 5-day constant infusions will have to be experimentally verified. The scheme, however, illustrates the value of pharmacokinetics as a tool which can be used to assist in the search for optimal delivery methods. ACKNOWLEDGMENTS We thank Dr. Ian Kerr and Dr. Luca Gianni for helpful discussions and Raymond Klecker for analytical assistance. REFERENCES 1. Alberts, D. S., Salmon, S. E., Chen, H-S. G., Moon, T. E., Young, L, and Survit, E. A. Pharmacologie studies of anticancer drugs with the human tumor stem cell assay. Cancer Chemother. Pharmacol., 6: 253-264,1981. 2. Andersson, B., Andersson, I., Beran, M., Ehrsson, H., and Eksborg, S. Liquid Chromatographie monitoring of daunorubicin and daunorubicinol in plasma from leukemic patients treated with daunorubicin or the daunorubicin DNA complex. Cancer Chemother. Pharmacol., 2:15-17, 1979. 3. Benet, L. Z., and Galeazzi, R. L. Noncompartmental determination of the steady-state volume of distribution. J. Pharm. Sci., 68:1071-1074,1979. 4. Benjamin, R. S. Clinical pharmacology of Adriamycin. Cancer Chemother. Rep., 6(Part III): 83-185, 1975. 5. Benjamin, R. S., Riggs, C. E., Jr., and Bachur, N. R. Pharmacokinetics and metabolism of Adriamycin in man. Clin. Pharmacol. Ther., 14:592-600,1973. JULY 6. Benjamin, R. S., Riggs, C. E., Jr., and Bachur, N. R. Plasma pharmacokinetics of Adriamycin and its metabolites in humans with normal hepatic and renal function. Cancer Res., 37: 1416-1420,1977. 7. Benjamin, R. S., Wiemik, P. H., and Bachur, N. R. Adriamycin chemotherapy: efficacy, safety, and pharmacological basis of an intermittent single highdosage schedule. Cancer (Phila.), 33:19-27,1974. 8. Blum, R. H., and Carter, S. K. Adriamycin: a new anticancer drug with significant clinical activity. Ann. Intern. Med., 80: 249-259, 1974. 9. Chan, K. K., Cohen, J. L., Gross, J. F., Himmelstein, K. J., Bateman, J. R., Tsu-Lee, Y., and Mariis, A. S. Prediction of Adriamycin disposition in cancer patients using a physiologic, pharmacokinetic model. Cancer Treat. Rep., 62: 1161-1171,1978. 10. Chlebowski, R. T., Chan, K. K., Tong, M. J., Weiner, J. M., Ryden, V. M. J., and Bateman, J. R. Adriamycin and methyl-CCNU combination therapy in hepatocellular carcinoma. Cancer (Phila.), 48:1088-1095,1981. 11. Creasey, W. A., Mclntosh, L. S., Brescia, T., Odujinrin, 0., Aspnes, G. T., Murray, E., and Marsh, J. C. Clinical effects and pharmacokinetics of different dosage schedules of Adriamycin. Cancer Res., 36: 216-221, 1976. 12. DiFronzo, G., Lenza, L., and Bonadonna, G. Distribution and excretion of Adriamycin in man. Biomedicine (Paris), 79:169-171,1973. 13. Drewinko, B., and Gottlieb, J. A. Survival kinetics of cultured human lymphoma cells exposed to Adriamycin. Cancer Res., 33:1141-1145,1973. 14. Eichholtz-Wirth, H. Dependence of the cytotoxic effect of Adriamycin on drug concentration and exposure time in vitro. Br. J. Cancer, 41: 886-891,1980. 15. Gibaldi, M., and Perrier, D. Pharmacokinetics. New York: Marcel Dekker, Inc., 1975. 16. Glazer, R. K., Hartman, K. D., and Richardson, C. L. Cytokinetic and biochem ical effects of 5-iminodaunorubicin in human colon carcinoma in culture. Cancer Res., 42: 117-121,1982. 17. Harris, P. A., and Gross, J. F. Preliminary pharmacokinetic model for Adria mycin (NSC-123127). Cancer Chemother. Rep., 59: 819-825, 1975. 18. Israel, M., Pegg, W. J., Wilkinson, P. J., and Gamick, M. B. Uquid Chromato graphie analysis of Adriamycin and metabolites in biological fluids. J. Liq. Chromatogr., 1: 795-809,1978. 19. Jusko, W. J. Pharmacodynamics of chemotherapeutic effects: dose-timeresponse relationships for phase-nonspecific agents. J. Pharm. Sci., 60: 892895,1971. 20. Knott, G. D., MLAB—A mathematical modeling tool. Comput. Programs Biomed., 10: 271-280, 1979. 21. Legha, S. S., Benjamin, R. S., Mackay, B., Ewer, M., Wallace, S., Valdivieso, M., Rassmussen, S. L., Blumenschein, G. R., and Freireich, E. J. Reduction of doxorubicin cardiotoxicity by prolonged continuous intravenous infusion. Ann. Intern. Med., 96:133-139,1982. 22. Ozols, R. F., Willson, J. K. V., Weltz, M. D., Grotzinger, K. R., Myers, C. E., and Young, R. C. Inhibition of human ovarian cancer colony formation by Adriamycin and its major metabolites. Cancer Res., 40: 4109-4112,1980. 23. Reich, S. D., Steinberg, F., Bachur, N. R., Riggs, C. E., Jr., Goebel, R., and Berman, M. Mathematical model for Adriamycin (doxorubicin) pharmacokinet ics. Cancer Chemother. Pharmacol., 3:125-131,1979. 24. Riggs, C. E., Jr., Benjamin, R. S., Serpick, A. A., and Bachur, N. R. Biliary disposition of Adriamycin. Clin. Pharmacol. Ther., 22: 234-241, 1977. 25. Wilkinson, P. M., and Mawer, G. E. The persistence of Adriamycin in man and rat. Br. J. Clin. Pharmacol., 1: 241-247,1974. 1983 Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1983 American Association for Cancer Research. 3421 Plasma Pharmacokinetics of Adriamycin and Adriamycinol: Implications for the Design of in Vitro Experiments and Treatment Protocols Raymond F. Greene, Jerry M. Collins, Jean F. Jenkins, et al. Cancer Res 1983;43:3417-3421. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/43/7/3417 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on April 29, 2017. © 1983 American Association for Cancer Research.