Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Conversion disorder wikipedia , lookup
History of psychosurgery in the United Kingdom wikipedia , lookup
Emergency psychiatry wikipedia , lookup
History of psychiatry wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Moral treatment wikipedia , lookup
Biology of depression wikipedia , lookup
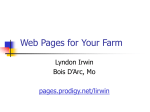
Fujita et al—cAMP Signaling in Brain is Decreased in Unmedicated Depressed Patients and Increased by Treatment with a Selective Serotonin Reuptake Inhibitor Supplementary Information Additional Descriptions on Participants. Major depressive disorder MDD patients were required to be free from psychotropic medications for at least two weeks before the baseline 11C(R)-rolipram PET scan (six weeks for fluoxetine). Healthy controls and patients were excluded if they had a history of alcohol or substance abuse within the past year or a lifetime history of alcohol or substance dependence based on DSM-IV. Herbal remedies or use of over-the-counter medications with known central nervous system effects were not permitted at any time during the study. MDD patients with serious suicidal ideation or psychosis were excluded from the study, but those with certain secondary anxiety disorders (generalized anxiety disorder, panic disorder, social phobia, anxiety disorder not otherwise specified, agoraphobia without panic disorder) were allowed to participate. In addition, we included patients with a remote history of posttraumatic stress disorder or obsessive-compulsive disorder but excluded subjects if these disorders were active at the time of enrollment. All participants underwent a urine drug screen for amphetamines, benzodiazepines, cocaine metabolites, opiates, and cannabinoids on the day of each 11C-(R)-rolipram PET scan. Participants were not allowed to ingest caffeine after midnight on the day before the PET scan. Statistical Analysis. Age, injection activity, and mass dose per body weight of 11C-(R)-rolipram were compared between the healthy control and MDD groups using Mann-Whitney U tests. For the patients who had two PET scans, injection activity and mass dose per body weight were compared between the two scans using Wilcoxon Signed Rank Tests. These nonparametric tests Page 1 of 4 were applied because the Shapiro-Wilk normality test indicated significant deviation from normal distribution. Clearance of 11C-(R)-rolipram from plasma was compared between controls and unmedicated patients using two-sample t-tests. For the patients who had two PET scans (unmedicated at baseline and after eight weeks of treatment with a selective serotonin reuptake inhibitor (SSRI)), clearance and changes in severity of symptoms were compared between the two scans using paired sample t-tests. Gender balance and percentage of cigarette smokers were compared between the two groups using Fisher’s exact test. VT/fP in the 10 brain regions was compared between control subjects and unmedicated MDD patients and between scans before and after starting SSRI using repeated measures two-way analysis of variance with regions as the within-subjects (repeating) factor. The repeated measures two-way analysis of variance was also performed to study the effect of cigarette smoking, prior medication, and current comorbid anxiety disorders. The selection of repeated measures two-way analysis of variance was used because the Shapiro-Wilk normality test did not indicate significant deviation of PET data from normal distribution. The effect size, Cohen’s d, was calculated by . For the PET scans in unmedicated patients at baseline, the correlation between each of the Montgomery Åsberg Depression Rating Scale (MADRS), 17-item Hamilton Rating Scale for Depression (HDRS-17), and Hamilton Scale for Anxiety (HAM-A) ratings and VT/fP in the 10 brain regions were investigated using Spearman’s bivariate correlation. In addition, the correlations were investigated after controlling for age (i.e., by partial correlation). For the patients who had two PET scans, the bivariate and partial correlation analyses were performed on the relationship between change in rating scale scores and VT/fP. The relationship between age and VT/fP was studied with both Pearson and Spearman methods. VT/fP in each voxel from control subjects and unmedicated MDD patients was compared using SPM8 two-sample t-tests. For both Page 2 of 4 baseline rolipram binding in each voxel and its changes after SSRI treatment, the relationship between rolipram binding and age was examined by an SPM8 regression model. The relationship between each of the MADRS, HDRS-17, and HAM-A ratings and VT/fP in each voxel of MDD patients was studied using an SPM8 regression model. All of the SPM analyses were performed with and without global normalization of proportional scaling. In the analyses that used binding in the 10 regions, P<.05 was considered statistically significant. In the SPM analyses, a family-wise error (FWE) corrected P<.05 was considered statistically significant. One-sided tests to both directions were applied in the SPM analysis to compare healthy controls and unmedicated patients. One-sided tests were applied to study correlations between rolipram binding and symptoms, and two-sided tests were applied in the other analyses. The statistical analyses were performed using IBM SPSS Statistics 22 (Armonk, New York) for data from the 10 regions or SPM8 for voxel data. Results are shown as mean ± SD. Parameters of 11C-(R)-rolipram scans PET scans were performed with similar injection activity for healthy controls (726±97 MBq), all unmedicated patients at baseline (714±90 MBq), and patients receiving SSRI treatment (737±38 MBq). No differences were observed between the groups (P>0.14). Mass dose was also similar between groups (healthy controls: 0.11±0.08, all unmedicated patients at baseline: 0.12±0.12, and patients taking an SSRI: 0.10±0.08 nmol/kg; P>0.30). At baseline, clearance did not significantly differ between healthy controls (181±83) and unmedicated patients (153±61 mL/min, P=0.084). It should be noted that even when clearance differed, rolipram binding measured as VT/fP from brain and arterial plasma data would not be affected by Page 3 of 4 clearance because the data acquisition was long enough to accurately measure equilibrium values 1 . No difference in clearance was observed between baseline and post-SSRI treatment scans (baseline: 157±68. SSRI: 165±63 mL/min. P=0.72). Changes in rolipram binding (Post SSRI - Base)/Base (%) Fig. S1. 100 50 0 -50 20 30 40 50 Age Relationship between age and change in 11C-(R)-rolipram binding after treatment with selective serotonin reuptake inhibitors (SSRIs). Older patients showed significantly greater increases in rolipram binding after treatment in 10 areas across brain (P<0.001, r=0.69–0.72). The graph shows average brain data from the 10 areas. References 1. Zanotti-Fregonara P, Zoghbi SS, Liow JS, Luong E, Boellaard R, Gladding RL et al. Kinetic analysis in human brain of [11C](R)-rolipram, a positron emission tomographic radioligand to image phosphodiesterase 4: a retest study and use of an image-derived input function. Neuroimage 2011; 54: 1903-1909. Page 4 of 4