Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
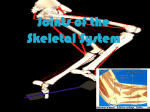
Arthrology of the Upper Limb Presented by David Rosenthal, DC, CSCS, BA, AS Click here for professional CV Resources: 1) 2) 3) 4) 5) 6) Main message: 1) 2) 3) Anatomy of Movement. (AM) Blandine Calais-Germaine (PT/dancer) Anatomy of Movement, The Exercises. BCG Atlas of Human Anatomy. Frank H. Netter. Clincally Oriented Anatomy, 3rd. ed. Keith L. Moore Color Atlas of Anatomy, 3rd ed. Rohen and Yokochi Upper extremity model from skeleton. Diagnoses and treatment always come back to the basic sciences: anatomy, physiology, neurology, biology, histology, microbiology, etc. If you know the normal structure and function, you will immediately know what abnormal is. If you know the anatomy, you can make up the technique that is appropriate for the dysfunctional tissue (Tufts University neurologist perspective). Lecture notes http:www.DavidRosenthalDC.com/chiropractic.html Encourage 1) 2) http://www.davidrosenthaldc.com/ Purchase models of tissue (like a full skeleton w/mm. attachments). To know what normal is. Use them every day in the office to express concepts and encourage follow through for care. Anatomy lab is an unbelievable opportunity to discover a world that few have the opportunity to. These people have donated themselves to give you an education. Find a part that interests you and fully dissect it in your free time in lab – i.e. superior sagittal sinus, sphenoid, AC jt., axilla, etc. VIII. Joints of the Upper Limb Introduction, General Movements: 6 types of Synovial joints (Please Put Sally Behind Her Cat): 1. Sternoclavicular Joint [G626;M784-fig. 6.59, N401-402(AM 106)] a. Articulation: “modified” saddle type, diarthrotic synovial jt. Fibrocartilage on ends of bones. Synovial joints are the most common and important type functionally) B. Articular Capsule Ligaments:thick capsule ant./post. with a interclavicular ligament and a costoclavicular lig. Has a fibrocartilaginous disc (NETTER 395/398, MOORE 3RD 609). c. Movements: of clavicle at this point(AM106) Anterior/posterior as scapula is protracted/retracted Superior/inferior as scapula is elevated/depressed Rotation d. Neurovascular Bundle:Internal thoracic artery(54 MOORE, 3RD ED)[comes directly off the subclavian artery] and medial supraclavicular nerve (790 Moore, 3rd ed.)[posterior to the SCM and anterior to the middle scalene](and n to subclavius) subclavius (AM116)is often a neglected mm – necessary in clinical evaluation. Has origin and insertion points – will affect blood supply to UE. Helpful in treating any disorder affecting he UE)[Hilton’s law-nerves supplying a joint also supply the muscles moving the joint and the skin covering the attachments of these mms.]) e. Clinicals: will fracture before it will dislocate on most occasions. As you will find with many of the ligamentous attachments – the density makes it often times stronger than bone. (Functional changes of this joint will affect the apices of the lungs and vascular affects to the UE) (SC is supported A&P by SCM) http://www.davidrosenthaldc.com/ 2. Acromioclavicular Joint [G627;M784-787; N406] a. Articulation: plane, diarthrotic synovial jt. Fibrocartilage on surfaces and angle of plane varies (S-C and AC BOTH fibrocartilagenous) (Moore 3rd Ed 609) b. Articular capsule / Ligaments: integrity of joint enhanced by the 2 part extrinsic coracoclavicular ligament(trapezoid lateral & conoid medial. Has incomplete fibrocartilagenous disc (NETTER 400) (Q: Which joint has an incomplete f-c disc?) c. Movements: sliding and gliding to slightly help ROM of shoulder complex d. Neurovascular bundle: suprascapular a with help from TA trunk branches(between SCM and anterior scalenes, posterior to the internal jugular vein (Moore 795 3rd ed.), nmostly lateral supraclavicular (Moore 790 3rd ed.)but some lateral pectoral and axillary (Netter 404). e. Clinicals: very common dislocation with clavicle passing superior to the acromial process of the scapula-referred to as “shoulder separation” (Effective treatment s/p injury is adjusting and KT (Kinesiotaping http://www.kinesiotaping.com). Will provide similar support as the integumentary system). http://www.davidrosenthaldc.com/ 3. Glenohumeral (shoulder) Joint [G628-630;M789-791; N406; AM 112-113] a. Articulation:ball & socket, diarthrotic synovial jt. Hyaline cartilage on shallow glenoid fossa & covering head of humerus. Glenoid fossa extended with figrocartilaginous labrum(like a toilet plunger seal). Joint sacrifices stability to gain ROM (stabilization exercises for teres minor/infraspinatus, teres major/subscapularis include lateral recumbents internal and external rotations with low weight and low reps). b. Articular Capsule / Ligaments/: capsule thickened in 3 places(which are all anterior). Coracohumeral lig. (Netter 398) aids joint capsule. Transverse humeral lig. (Netter 398) helps hold tendon of long head of biceps in place c. Bursae: Subacromial(subdeltoid) bursa (N 398) which is anterior to the subscapularis mm. Subscapular bursa (Moore’s 3rd 610) which blends in with synovial membrane of articular capsule and is posterior inferior to the coracoid and subscapularis mm . d. Movements / Scapulothoracic articulation:flex/ext, ab/adduction, int/ext rotation(med/lat) and circumduction. With abduction the scapula must begin moving as you exceed 90°(scapulothoracic artic.) (AM 119 scapular movement) f. Neurovascular Bundle: Suprascapular a (Netter 404) & ant/post humeral circumflex aa(Netter 404), Hilton’s Law: Suprascapular(trunk C5-6), Axillary(terminal branch C5-6) (Ne.405) Lat. Pectoral(cord C5-7) are main nerves. (Brachial plexus memorize for boards) http://www.davidrosenthaldc.com/ g. Clinical: Calcium deposits(hydroxyapatite), rotator cuff tears, dislocation(usually anterior & inferior), labrum damage. (labral tears can be difficult to diagnose, need MRI – best to refer earlier than later). Women who are smaller framed, peri-menopausal and elderly have greater chance of frank dislocation). (Clinical evaluation important to look at support system of the supraspinatus, infraspinatus, teres minor, teres major, subscapularis, sublclavius and the most neglected mm in UE management – the pectoralis minor,with it’s 3 insertion points on ribs 3,4 and 5). (Make sure you learn how to re-set a dislocated shoulder – it’s an easy procedure and done most effectively as soon as the injury occurs [ligament creep doesn’t set in]. There is less likelihood of vascular damage – always determine radial and ulnar pulses along with capillary bed re-vascularization at the nail beds). Ligament of Struthers is often neglected in management of CTS Ligament of Struthers 4. Elbow Joint [G681-682;M795-802; N419, 421] a. Articulation: hinge, diarthrotic synovial jt. Hyaline cart.(not a great deal of weight bearing on that joint surface). b. Articular Capsule / Ligaments: capsule strengthened by medial/lateral(radial/ulnar) collateral ligs (Netter 412). Medial hd. of triceps and brachialis blend into capsule to “lift” it out of harms way c. Movements:flexion/extension(multiple small bursa) (although pronation and supination is provided by muscles with origins of the medial and lateral condyle Netter 414-5.) d. Neurovascular Bundle: from brachial, radial and ulnar aa(collaterals and recurrents), Hilton’s Law: radial, ulnar and musculocutaneous(and even some median) (Netter 408, 409, 412). e. http://www.davidrosenthaldc.com/ Clinicals: Carrying angle (women make better receivers in volleyball because of an increased CA), bursitis, valgus/varus (AM 137) Females: 5 degrees, Male: 10-15 degrees. 5. Proximal/distal radioulnar joint(N 421-422) pivot type synovial jt. Annular ligament(like a sling – AM 135) holds head of radius in place. Oblique cord limits supination. Interosseous membrane (Netter 413) makes the intact unit a syndesmosis type joint. United by fibrous tissue. Interosseous membrane mobilization makes a significant impact in carpal tunnel syndrome) 6. Wrist Joint[ N437-438] a. Articulation:condyloid type, diarthrotic synovial jt. (Netter 426-427). b. Articular Capsules / Ligaments: thickened on all four sides. Has a fibrocartilagenous disc (Netter 427) from radius to ulna separating head of ulna from lunate and triquetral bone c. Movements:flexion/extension, ab/aduction (radial and ulnar deviation), & circumduction. d. Neurovascular Bundle: radial/ulnar aa, median, radial and ulnar nn(Hilton’s Law) e. Clinicals: effect of anteriorly displaced lunate on median nerve. CTS with a multitude of causes from restrictions http://www.davidrosenthaldc.com/ 7. Intercarpal Joints[N 441]-plane gliding , synovial jts. Many ligaments (I encourage you to try and dissect one of the carpals out of the ligamentous mass). AM 150 gliding joints. 8. Carpometacarpal / Intermetacarpal Joints: Netter 430 with the exception of thumb these are all plane, synovial joints. The trapezium to 1st metacarpal is a saddle joint(ext/flex,ab/ad,opp,circum) (AM150). 9. Metacarpophalangeal / Interphalangeal Joints (Netter 431) Metacarpophalangeal-condyloidext/flex,ab/ad,circumduction Interphalangeal-hinge type-ext/flex http://www.davidrosenthaldc.com/