Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
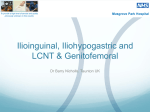
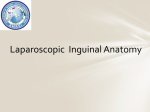
Anatomy Block 5 Oral Quiz Review 3/3/2013 12:08:00 AM Teach or demonstrate the following: 1.) The four layers of the abdominal fascia 1. Superficial Fascia (Camper’s)=fatty, subcutaneous fascia 2. Membranous fascia (Scarpa’s) = deeper membranous fat 3. Deep Investing Fascia = ‘felt’ fascia that covers the abdominal muscles 4. Endoabdominal Fascia = fascia of the transversalis muscle Note: arcuate line differences 2.) The four muscles of the abdominal wall 1. Rectus abdominus a. Paired muscles that run vertically i. Origin – Pubis ii. Insertion – Costal cartilages 5-7, xiphoid process iii. Innervation – (T7-T12) segmental nerves iv. Action – Flexion of the lumbar spine 2. Transversus abdominus a. Muscle of the lateral & anterior abdomen b. Horizontal (transverse) fibers & deepest muscle layer i. Origins Iliac crest Inguinal ligament Thoracolumbar fascia Costal cartilages 7-12 ii. Insertions Xiphoid, linea alba Pubic crest & pectin pubis via conjoint tendon iii. Innervation Thoracoabdominal nn. (T6-T11) Subcostal nerve (T12) Iliohypogastric nerve (L1) Ilioinguinal nerve (L1) iv. Action – Compresses abdominal contents 3. External oblique a. Largest, most superficial abdominal muscle b. ‘Hands in pockets’ fiber direction i. Origin – Ribs 5-12 ii. Insertions Iliac crest Pubic tubercle Linea alba iii. Innervation Thoracoabdominal nn. (T7-T11) Subcoastal nerve (T12) iv. Action – contralateral rotation of the torso 4. Internal oblique a. Rotate your ‘hands in pockets’ 90° b. Inferior layer to external oblique i. Origin Inguinal ligament Iliac crest Thoracolumbar fascia ii. Insertions Linea alba Pectin pubis (via conjoint tendon) Ribs 10-12 iii. Innervation Thoracoabdominal nn. (T6-T11) Subcostal nerve (T12) Iliohypogastric nerve (L1) Ilioinguinal nerve (L1) iv. Action Compresses abdomen Unilateral contraction will rotate vertebral column ispilaterally 3.) The organization of the neurovascular bundles in the abdominal wall and relate these structures to back, flank and anterior abdominal wall pain. When considering pain of the lower back, flank, or anterior abdomen, one should know that the dermatomal map of the anterolateral abdomen is almost identical to the distribution of peripheral nerves. The spinal levels T7-T12 do not participate in plexus formation. The exception to this rule is at the L1 level (iliohypogastric & ilioinguinal). Here, the dermatome has two peripheral nerves and explains why a swift kick to Sam Sauce’s nuts will also elicit epigastric pain. Between the internal oblique and transversus abdominis muscles is a neurovascular plane, which corresponds with a similar plane in the intercostal spaces. In both regions, the plane lies between the middle and deepest layers of muscle. The neurovascular plane of the anterior abdominal wall contains nerves and arteries supplying anterolateral abdominal wall. In the anterior part of abdominal wall, nerves and vessels leave neurovascular plane and lie mostly in subcutaneous tissue (Moore’s 191). This photo is sort of helpful and sort of hilarious. 4.) Describe the four routes of the venous drainage of the anterior and posterior abdominal wall 1. Superior epigastric vein & branches of musculophrenic vein to the internal thoracic o to the subclavian 2. Inferior epigastric vein & deep circumflex iliac vein to the external iliac vessels 3. Superficial circumflex iliac vein & superficial epigastric vein to the femoral vein 4. Posterior intercostal vein of 11th intercostal space & anterior branches of the subcostal veins to the azygos/hemiazygos system 5.) The five umbilical peritoneal folds The peritoneal folds refer to the five, one unpaired and two paired, foldings in the anterior peritoneum (1) Median umbilical fold o overlies the median umbilical ligament extends from bladder’s apex to umbilicus (2) Medial umbilical folds o overlie the occluded remains of umbilical arteries (2) Lateral umbilical folds o overlie the inferior epigastric vessels o only fold that’s over a functioning adult structure o extends from the inguinal ring to the arcuate line o 6.) The borders of the inguinal canal and its contents; relate these structures to direct and indirect inguinal hernias and to focal and diffuse abdominal pain The inguinal canal passes obliquely through the lower abdominal wall, extending between the superficial and deep inguinal rings. The borders of the canal are Anterior: aponeurosis of external oblique, fleshy internal oblique Superior: Medial crus of ext obl., musculoaponeurotic arches of internal oblique & transverse abdominus, transversalis fascia Posterior: Transversalis fascia, conjoint tendon (medial), and deep inguinal ring (lateral) Inferior: Inguinal ligament, lacunar ligament (medial), iliopubic tract (lateral) Contents are Male o Spermatic cord Vas deferens Ilioinguinal nerve Genital branch of genitofemoral nerve Testicular arteries/veins Pampiniform plexus Lymph vessels Cremaster muscle Female o Round ligament of the uterus o Ilioinguinal nerve o Lymph vessels Direct hernia Passes directly through the abdominal wall (Hesselbach’s Δ) to the superficial inguinal ring, forming peritoneal sac o Linea semilunaris (lateral rectus border) o Inferior epigastric vessels o Inguinal ligament Due to muscular weakness or increased intrabdominal pressure More common in aging men Indirect Does not extend to scrotum hernia Traverses the superficial, deep inguinal rings Is within the covering of spermatic cord May descend into scrotum can be congenital, common in younger males 7.) The location of the kidney, adrenal gland, urinary pelvis and ureter on a human and on an abdominal plain film and relate these structures to the presentation of flank pain Along mid-clavicular line Left kidney: T12-L3 Right Kidney: T12.5-L3.5 Pelvis’: L1-L2 Adrenals: T11 The ureters emerge ~L2 and descend in parallel (approx. linea semilunaris) and hit the bladder, which is midline, just superior to the pubis and inguinal ligaments. On abdominal plain film: P – renal pelvis * - ureter B – bladder Adrenals – unmarked K - kidney 3/3/2013 12:08:00 AM 3/3/2013 12:08:00 AM