Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Neonatal infection wikipedia , lookup
DNA vaccination wikipedia , lookup
Immunocontraception wikipedia , lookup
Infection control wikipedia , lookup
Vaccination policy wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Vaccination wikipedia , lookup
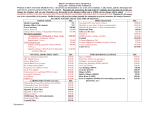
◄ STAPLE copy of Hepatitis B Surface Antibody (anti-HBs) titer lab results here! Department of Dental Education 260-481-6837 NAME Date__________________ IPFW ID# PROGRAM: ____Dental Assisting ____Dental Hygiene ____Dental Laboratory Technology Directions: Use either Section A or Section B and complete the bottom portion of the page. Section A: HEPATITIS IMMUNIZATION RECORD HepB Vaccination Dates: Hepatitis B Surface Antibody Anti-HBs Titer Results: (test 1-2 mo. later) 1.____________________(initial) Titer Date__________________ 2.____________________(1 mo. later) Results____________________ 3.____________________(5 mo. later) *attach copy of results and submit to Neff Hall, suite 150 ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Section B: HEPATITIS B VACCINATION DECLINATION I understand that due to my chance of occupational exposure to blood or other potential infectious materials I may be at risk of acquiring Hepatitis B infection. At this time I choose not to receive the Hepatitis B vaccine. Reason: _______________________________________________________________________ Therefore, Indiana University-Purdue University Fort Wayne, the Department of Dental Education, or its allied dental programs will not be responsible if I should acquire Hepatitis B. Signed Date