Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
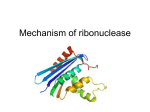
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Cancer Prone Disease Section Review Cartilage-hair hypoplasia (CHH) Pia Hermanns, Brendan Lee Department of Molecular and Human Genetics, Howard Hughes Medical Institute, Baylor College of Medicine, One Baylor Plaza Room 635E, Mail Stop 225, Houston, TX 77030, USA Published in Atlas Database: October 2007 Online updated version: http://AtlasGeneticsOncology.org/Kprones/CartilageHairHypoID10105.html DOI: 10.4267/2042/38617 This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 2008 Atlas of Genetics and Cytogenetics in Oncology and Haematology Treatment Identity Other names: Metaphyseal McKusick type Inheritance: Autosomal rezessive. - Disproportionate short stature: Treatment with growth hormone is likely not beneficial in children with CHH. Surgical bone lengthening is occasionally considered. - Orthopedic problems: The lumbar lordosis and ligamentous laxity can cause joint pains of the lower spine, the knees and ankles. - Immunodeficiency: The cellular immunity may be defective whereas the humoral immunity is usually intact. However, there are a few cases that have combined immune deficiency. - Vaccination: immunization with live vaccines is contraindicated in patients with impaired cellular immunity. - Anemia: Patients with severe anemia (5% of CHH patients) require repeated transfusions. A few cases might need lifelong transfusions and/or bone marrow transplantation. - Gastrointestinal dysfunction: This can present with signs of malabsorption, diarrhea, celiac disease, and failure to thrive. This requires symptomatic treatment. It also may present as Hirschsprung¹s disease that can be surgically corrected. - Malignancies: Patients should be monitored closely, since they have a higher risk of developing lymphomas and leukemias. chondrodysplasia, Clinics Note: CHH was first described in the Amish, an isolated religious group in the USA by Victor McKusick in 1965. It is a multi-systemic disorder characterized by short stature, blond fine sparse hair, but this may be quite variable, and defective cellular immunity predominantly affecting T-cell mediated responses. Patients may have severe combined immunodeficiency, requiring bone marrow transplantation or they may be asymptomatic. Gastrointestinal dysfunctions are frequently observed such as mal-absorption or Hirschsprung¹s disease. The incidence of CHH in the Amish is 1.5 in 1,000 births, whereas in Finland it is 1 in 18,000 to 23,000 live births. Phenotype and clinics The metaphyses of tubular bones are widened, scalloped and irregularly sclerotic. Delayed ossification and trabeculation of the long bones are also characteristic findings on X-rays. All long bones are affected. The relative length of the humerus, ulna, radius, tibia and fibula decreases rapidly in early childhood and again at puberty. Relatively short and broad phalanges of the hands are observed. Prognosis Adult height ranges between 111 and 151 cm in males and between 104 and 137 cm in females. No more than 20% of CHH patients exhibit recurrent and severe infections. These patients show evidence of immune deficiency in vivo and in vitro. Neoplastic risk A predisposition to certain lymphomas has been reported. cancers Atlas Genet Cytogenet Oncol Haematol. 2008;12(6) primarily 481 Cartilage-hair hypoplasia (CHH) Hermanns P, Lee B (violet), an octamer (olive green), a proximal sequence element (PSE) (turquoise) and a TATA box (red). Genes involved and Proteins Transcription: In vitro analysis of the RMRP promoter revealed that the four described promoter elements are sufficient for RMRP transcription. It is transcribed by the DNA dependent RNA polymerase III and is encoded in the nucleolus. The complex is localized primarily in the nucleolus and to a lesser extend in the mitochondria. Studies in yeast revealed multiple functions of this protein complex. RNase MRP is involved in mitochondrial DNA replication by cleaving the RNA primer starting mitochondrial replication and is also involved in the RNA primer formation itself. In addition it plays a role in cell cycle progression at the end of mitosis. RNase MRP cleaves the 5’ UTR of the CLB2 gene thus causing a rapid CLB2 degradation, which leads to a cell cycle progression. If CLB2 is not cleaved cell cycle will be arrest. The best understood function is its processing of pre-ribosomal RNAs. It cleaves the pre-ribosomal RNA at the A3 site thus helping in the maturation of the short and active form of the 5.8S rRNA. Note: CHH is mainly caused by mutations in the RMRP gene, but a Uniparental Disomy of 9p13 has been reported as well in one CHH patient. RMRP (RNA component of Mitochondrial RNA-Processing endoribonuclease) Location: 9p13 DNA/RNA RMRP is the RNA component of the RNase MRP protein complex. It functions as an RNA and is not translated into a protein. The RMRP gene is an intronless gene, that is 267 bp long (blue). The promoter region contains a SP1 binding site Atlas Genet Cytogenet Oncol Haematol. 2008;12(6) 482 Cartilage-hair hypoplasia (CHH) Hermanns P, Lee B Protein Expression: Strong ubiquitous expression in mouse embryos (E9.5 to E18.5 have been tested) and in adult animals. In bone Rmrp is more strongly expressed in hypertrophic chondrocytes and pericondrium than in the zone of proliferating chondrocytes. There is also very strong expression in the epiphysis. In Xenopus laevis oocytes RMRP is stronger expressed in developmental stages with a higher content of mitochondria. Function: The RNase MRP complex is highly conserved among a variety of different species (human, mouse, rat, cow, frog, yeast and plants). Homology The functional analysis of the RNase MRP endoribonuclease is complicated by the fact, that eight proteins are shared by a related ribonucleoprotein complex, called RNase P. RNase P is also a ribonucleprotein endoribonuclease and is mainly involved in rRNA precursor maturation. Atlas Genet Cytogenet Oncol Haematol. 2008;12(6) Mutations The most frequently found mutation among CHH patients is a 70 A to G transition mutation with an ancient founder origin established in Finland, a country where the disorder is uncommonly frequent. In fact it is the only mutation found in Amish CHH patients. Over 93 different mutations have been described in CHH patients. These include promoter duplications, triplications and insertions exclusively between the TATA box and the transcription start site. These mutations decrease the RMRP transcription efficiency. Single base pair substitutions are spread out over the entire RMRP transcript. Also small deletions of and insertions in the transcribed region of the gene have been observed as well. These mutations might influence the secondary structure of the RNA, the binding of the proteins to the RNA or the RNA stability. In addition many polymorphisms and rare sequence variants have been observed. This is remarkable considering the very small size of the RMRP gene. 483 Cartilage-hair hypoplasia (CHH) Hermanns P, Lee B hypoplasia variant with only skeletal manifestations and reveals a high density of single-nucleotide polymorphisms. Clin Genet 2002;61(2):146-151. To be noted So far no complete deletion of the entire RMRP gene has been observed. This suggests that complete loss of RMRP function might be incompatible with life. This is also supported by the fact that the knock out in yeast is lethal. Cai T, Aulds J, Gill T, Cerio M, Schmitt ME. The Saccharomyces cerevisiae RNase mitochondrial RNA processing is critical for cell cycle progression at the end of mitosis. Genetics 2002;161(3):1029-1042. Mäkitie O, Heikkinen M, Kaitila I, Rintala R. Hirschsprung's disease in cartilage-hair hypoplasia has poor prognosis. J Pediatr Surg 2002;37(11):1585-1588. References Ridanpää M, Sistonen P, Rockas S, Rimoin DL, Mäkitie O, Kaitila I. Worldwide mutation spectrum in cartilage-hair hypoplasia: ancient founder origin of the major70 A--->G mutation of the untranslated RMRP. Eur J Hum Genet 2002;10(7):439-447. McKusick VA, Eldridge R, Hostetler JA, Ruangwit U, Egeland JA. Dwarfism in the Amish. II Cartilage-Hair Hypoplasia. Bull Johns Hopkins Hosp 1965;116:285-326. Berthet F, Siegrist CA, Ozsahin H, Tuchschmid P, Eich G, Superti-Furga A, Seger RA. Bone marrow transplantation in cartilage-hair hypoplasia: correction of the immunodeficiency but not of the chondrodysplasia. Eur J Pediatr 1996;155(4):286-290. Nakashima E, Mabuchi A, Kashimada K, Onishi T, Zhang J, Ohashi H, Nishimura G, Ikegawa S. RMRP mutations in Japanese patients with cartilage-hair hypoplasia. Am J Med Genet A 2003;123(3):253-256. Kooijman R, van der Burgt CJ, Weemaes CM, Haraldsson A, Scholtens EJ, Zegers BJ. T cell subsets and T cell function in cartilage-hair hypoplasia. Scand J Immunol 1997;46(2):209215. Ridanpää M, Jain P, McKusick VA, Francomano CA, Kaitila I. The major mutation in the RMRP gene causing CHH among the Amish is the same as that found in most Finnish cases. Am J Med Genet C Semin Med Genet 2003;121(1):81-83. Sulisalo T, Mäkitie O, Sistonen P, Ridanpää M, el-Rifai W, Ruuskanen O, de la Chapelle A, Kaitila I. Uniparental disomy in cartilage-hair hypoplasia. Eur J Hum Genet 1997;5(1):35-42. Bonafé L, Dermitzakis ET, Unger S, Greenberg CR, CamposXavier BA, Zankl A, Ucla C, Antonarakis SE, Superti-Furga A, Reymond A. Evolutionary comparison provides evidence for pathogenicity of RMRP mutations. PLoS Genet 2005;1(4):e47. Giedion A. Phalangeal cone-shaped epiphyses of the hand: their natural history, diagnostic sensitivity, and specificity in cartilage hair hypoplasia and the trichorhinophalangeal syndromes I and II. Pediatr Radiol 1998;28(10):751-758. Hermanns P, Bertuch AA, Bertin TK, Dawson B, Schmitt ME, Shaw C, Zabel B, Lee B. Consequences of mutations in the non-coding RMRP RNA in cartilage-hair hypoplasia. Hum Mol Genet 2005;14(23):3723-3740. Mäkitie O, Kaitila I, Savilahti E. Susceptibility to infections and in vitro immune functions in cartilage-hair hypoplasia. Eur J Pediatr 1998;157(10):816-820. Thiel CT, Horn D, Zabel B, Ekici AB, Salinas K, Gebhart E, Rüschendorf F, Sticht H, Spranger J, Müller D, Zweier C, Schmitt ME, Reis A, Rauch A. Severely incapacitating mutations in patients with extreme short stature identify RNAprocessing endoribonuclease RMRP as an essential cell growth regulator. Am J Hum Genet 2005;77(5):795-806. Glass RB, Tifft CJ. Radiologic changes in infancy in McKusick cartilage hair hypoplasia. Am J Med Genet 1999;86(4):312315. Mäkitie O, Pukkala E, Teppo L, Kaitila I. Increased incidence of cancer in patients with cartilage-hair hypoplasia. J Pediatr 1999;134(3):315-318. Williams MS, Ettinger RS, Hermanns P, Lee B, Carlsson G, Taskinen M, Mäkitie O. The natural history of severe anemia in cartilage-hair hypoplasia. Am J Med Genet A 2005;138(1):3540. Yel L, Aggarwal S, Gupta S. Cartilage-hair hypoplasia syndrome: increased apoptosis of T lymphocytes is associated with altered expression of Fas (CD95), FasL (CD95L), IAP, Bax, and Bcl2. J Clin Immunol 1999;19(6):428-434. Hermanns P, Tran A, Munivez E, Carter S, Zabel B, Lee B, Leroy JG. RMRP mutations in cartilage-hair hypoplasia. Am J Med Genet A 2006;140(19):2121-2130. Mäkitie O, Juvonen E, Dunkel L, Kaitila I, Siimes MA. Anemia in children with cartilage-hair hypoplasia is related to body growth and to the insulin-like growth factor system. J Clin Endocrinol Metab 2000;85(2):563-568. Hirose Y, Nakashima E, Ohashi H, Mochizuki H, Bando Y, Ogata T, Adachi M, Toba E, Nishimura G, Ikegawa S. Identification of novel RMRP mutations and specific founder haplotypes in Japanese patients with cartilage-hair hypoplasia. J Hum Genet 2006;51(8):706-710. Mäkitie O, Kaitila I, Pukkala E, Teppo L, Savilahti E. The role of immune deficiency in cartilage-hair hypoplasia. Duodecim 2000;116(12):1299-1308. Muñoz-Robles J, Allende LM, Clemente J, Calleja S, Varela P, Gonzalez L, de Pablos P, Paz E, Morales P. A novel RMRP mutation in a Spanish patient with cartilage-hair hypoplasia. Immunobiology 2006;211(9):753-757. Mäkitie O, Kaitila I, Savilahti E. Deficiency of humoral immunity in cartilage-hair hypoplasia. J Pediatr 2000;137(4):487-492. Mäkitie O, Kaitila I, Rintala R. Hirschsprung disease associated with severe cartilage-hair hypoplasia. J Pediatr 2001;138(6):929-931. Martin AN, Li Y. RNase MRP RNA and human genetic diseases. Cell Res 2007;17(3):219-226. Mäkitie OM, Tapanainen PJ, Dunkel L, Siimes MA. Impaired spermatogenesis: an unrecognized feature of cartilage-hair hypoplasia. Ann Med 2001;33(3):201-205. Thiel CT, Mortier G, Kaitila I, Reis A, Rauch A. Type and Level of RMRP Functional Impairment Predicts Phenotype in the Cartilage Hair Hypoplasia - Anauxetic Dysplasia Spectrum. Am J Med Genet 2007;81(3):519-529. Ridanpää M, van Eenennaam H, Pelin K, Chadwick R, Johnson C, Yuan B, vanVenrooij W, Pruijn G, Salmela R, Rockas S, Mäkitie O, Kaitila I, de la Chapelle A. Mutations in the RNA component of RNase MRP cause a pleiotropic human disease, cartilage-hair hypoplasia. Cell 2001;104(2):195-203. This article should be referenced as such: Hermanns P, Lee B. Cartilage-hair hypoplasia (CHH). Atlas Genet Cytogenet Oncol Haematol.2008;12(6):481-484. Bonafé L, Schmitt K, Eich G, Giedion A, Superti-Furga A. RMRP gene sequence analysis confirms a cartilage-hair Atlas Genet Cytogenet Oncol Haematol. 2008;12(6) 484