Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
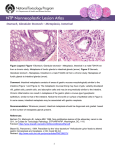
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Leukaemia Section Mini Review Myelofibrosis with myeloid metaplasia (MMM), Idiopathic myelofibrosis, Agnogenic myeloid metaplasia Antonio Cuneo, Francesco Cavazzini Hematology Section, Department of Biomedical Sciences, University of Ferrara, Corso Giovecca 203, Ferrara, Italy Published in Atlas Database: August 2006 Online updated version: http://AtlasGeneticsOncology.org/Anomalies/Myelofib.html DOI: 10.4267/2042/38381 This article is an update of: Huret JL. Myelofibrosis with myeloid metaplasia (MMM). Agnogenic myeloid metaplasia. Atlas Genet Cytogenet Oncol Haematol.1998;2(1):17. This work is licensed under a Creative Commons Attribution-Non-commercial-No Derivative Works 2.0 France Licence. © 2007 Atlas of Genetics and Cytogenetics in Oncology and Haematology As the disease progresses, increased marrow fibrosis with severe symptomatic peripheral cytopenias and extramedullary hemopoiesis predominate, with consequent massive splenomegaly, hepatomegaly with portal hypertension, pulmonary hypertension. Leukemic transformation may represent the terminal event in 5-20% of the cases. Clinics and pathology Disease Chronic myeloproliferative disorder Phenotype / cell stem origin The disease is a chronic myeloproliferative disorder originating from a mutated pluripotent stem cell capable of producing red blood cells, granulocytes, megakaryocytes and lymphoid cells. Fibrosis of the marrow is the hallmark of the disease, however fibroblasts are not part of the malignant process and fibrosis represents a reaction of marrow stromal cells. Cytology Teardrop poikilocytosis and leukoerythroblastosis are present in the peripheral blood (PB) smear. Platelet are increased in size. The bone marrow is usually hypercellular at presentation with remarkably increased megakaryocytes and, to a lesser degree, granulocytes. Reticulin fibrosis is always present. Hemopoietic cellularity is patchy, with some areas showing hypercellularity and other being depleted of hemopoietic cells. The spleen histology shows extramedullary hemopoiesis involving predominantly the sinusoids. Epidemiology MMM has an incidence of 0.3 to 1.5 new cases per year in 100.000 persons. Male predominance was observed in some studies and not confirmed in others. The average age at diagnosis is 60 years. Exposure to radiation and to organic solvents increases the risk of developing MMM. Treatment Clinics The treatment depends on the patient’s general condition and symptoms. Supportive treatment is required for anemia and profound thrombocytopenia. Cytoreductive treatment with busulphan, hydroxyurea, thioguanine, low-dose melphalan or chlorambucil, interferon-a may be useful to control progressive splenomegaly. Irradiation of the spleen may be also employed. Danazol or low-dose dexamethasone can be used to ameliorate anemia. Allogeneic bone marrow transplantation should be considered for patients aged 60 years or less. MMM usually presents with fatigue, weight loss, splenomegaly with or without symptoms. Anemia and various alterations of the white blood cell and/or platelet count are frequently seen at diagnosis. Thrombocytopenia-related bleeding may occur. MMM must be distinguished from myelodysplasia with fibrosis, from acute megakayoblastic leukemia and acute myelofibrosis. Atlas Genet Cytogenet Oncol Haematol. 2007;11(1) 27 Myelofibrosis with myeloid metaplasia (MMM), Idiopathic myelofibrosis, Agnogenic myeloid metaplasia progenitors in PV are hypersensitive to stimulation by these cytokines. Patients with JAK2 V617F mutation showed high white blood cell counts, required less transfusions and had an inferior outcome in a study. In 5-9% of the patients a gain-of-function mutation of the thrombopoietin receptor (MPL) gene can be found, determining activation of the JAK-STAT pathway. Prognosis The median survival is approximately 5 years. Causes of death include infection, leukemic transformation, bleeding, hepatic failure with portal hypertension due to myeloid metaplasia, heart failure. Cytogenetics Cytogenetics morphological References a) Chromosome lesions: The absence of the t(9;22)/BCR-ABL fusion is an absolute diagnostic requirement. Approximately 4050% of the patients analyzed at diagnosis show a clonal defect. The proportion of cytogenetically abnormal cases increases at disease transformation into acute leukemia, were up to 90% of the cases carry a clonal defect. Non-random chromosome aberrations are del(13q), del(20q) and gain of 1q. These abnormalities represented 65% of abnormal cases in a study. Other recurrent chromosome aberrations include trisomy 8 and del(12p), monosomy 7/del(7q), der(6)t(1;6)(q2123;p21.3). The latter abnormality leads to trisomy 1q21-23 to 1qter and to loss of 6p21 to 6pter. FISH on deparaffinized bone biopsies showed a 56% incidence of cytogenetic lesions in a study using probes for 7q31, 12p, 13q14, 17p13, 20q13, 21q22, cen7, cen8, cen11 and cen17. b) Prognostic significance: The presence of abnormal karyotype does not appear to be an independent prognostic factor, whereas +8, 12p deletion and -7/7q- were associated with an inferior outcome at multivariate analysis. Reilly JT, Snowden JA, Spearing RL, Fitzgerald PM, Jones N, Watmore A, Potter A. Cytogenetic abnormalities and their prognostic significance in idiopathic myelofibrosis: a study of 106 cases. Br J Haematol 1997;98:96-102. Tefferi A, Mesa RA, Schroeder G, Hanson CA, Li CY, Dewald GW. Cytogenetic findings and their clinical relevance in myelofibrosis with myeloid metaplasia. Br J Haematol 2001;113:763-771. Bacher U, Haferlach T, Kern W, Hiddemann W, Schnittger S, Schoch C. Conventional cytogenetics of myeloproliferative diseases other than CML contribute valid information. Ann Hematol 2005;84:250-257. Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N, Swanton S, Vassiliou GS, Bench AJ, Boyd EM, Curtin N, Scott MA, Erber WN, Green AR. Cancer Genome Project. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet 2005;365:1054-1061. Dingli D, Grand FH, Mahaffey V, Spurbeck J, Ross FM, Watmore AE, Reilly JT, Cross NC, Dewald GW, Tefferi A. Der(6)t(1;6)(q21-23;p21.3): a specific cytogenetic abnormality in myelofibrosis with myeloid metaplasia. Br J Haematol 2005;130:229-232. Hoffman R, Ravandi-Kashani F, IN: Hoffman R, Benz EJ, Shattil SJ, Furie B, Cohen HJ, Silbertsein LE, McGlave P (Eds). Idiopathic myelofibrosis. Hematology. Basic Principles and practice. Elsevier, Philadelphia, Pennsylvania, 2005 pp1255-1275. Genes involved and Proteins Mesa RA, Li CY, Ketterling RP, Schroeder GS, Knudson RA, Tefferi A. Leukemic transformation in myelofibrosis with myeloid metaplasia: a single-institution experience with 91 cases. Blood 2005;105:973-977. JAK2 Location: 9p24 Note: Janus Kinase JAK2 mutation (See also Polycythemia Vera). Protein A valine to phenylalanine substitution at position 617 (JAK2 V617F mutation) is present in approximately 50-55% of the patients leading to constitutive kinase activity. The mutated JAK2 protein binds to the cytoplasmic domain of Epo-R and promotes signalling independent of Epo stimulation. The JAK2 protein is coded for by a gene mapping at 9p and it is activated upon erythropoietin binding to the receptor. JAK2 signalling involves the phosphorylation of several Y residues at the Epo receptor with activation of STAT, MAP kinase PI-3-kinase and AKT. These events lead to survival and proliferation of erythroid progenitors. JAK2 is involved in intracellular signalling following stimulation by IL3, TPO and GM-CSF, and erythroid Atlas Genet Cytogenet Oncol Haematol. 2007;11(1) Cuneo A, Cavazzini F Strasser-Weippl K, Steurer M, Kees M, Augustin F, Tzankov A, Dirnhofer S, Fiegl M, Gisslinger H, Zojer N, Ludwig H. Chromosome 7 deletions are associated with unfavorable prognosis in myelofibrosis with myeloid metaplasia. Blood 2005;105:4146. Vainchenker W. Constantinescu SN. A Unique Activating Mutation in JAK2 (V617F) Is at the Origin of Polycythemia Vera and Allows a New Classification of Myeloproliferative Diseases. ASH Educational Book 2005:195-200. Campbell PJ, Griesshammer M, Döhner K, Döhner H, Kusec R, Hasselbalch HC, Larsen TS, Pallisgaard N, Giraudier S, Le Bousse-Kerdilès MC, Desterke C, Guerton B, Dupriez B, Bordessoule D, Fenaux P, Kiladjian JJ, Viallard JF, Brière J, Harrison CN, Green AR, Reilly JT. V617F mutation in JAK2 is associated with poorer survival in idiopathic myelofibrosis. Blood 2006;107:2098-2100. Pardanani AD, Levine RL, Lasho T, Pikman Y, Mesa RA, Wadleigh M, Steensma DP, Elliott MA, Wolanskyj AP, Hogan WJ, McClure RF, Litzow MR, Gilliland DG, Tefferi A. MPL515 mutations in myeloproliferative and other myeloid disorders: a study of 1182 patients. Blood 2006;108(10):3472-3476. Pikman Y, Lee BH, Mercher T, McDowell E, Ebert BL, Gozo M, Cuker A, Wernig G, Moore S, Galinsky I, Deangelo DJ, Clark JJ, Lee SJ, Golub TR, Wadleigh M, Gilliland DG, Levine RL. 28 Myelofibrosis with myeloid metaplasia (MMM), Idiopathic myelofibrosis, Agnogenic myeloid metaplasia MPLW515L Is a Novel Somatic Activating Mutation in Myelofibrosis with Myeloid Metaplasia. PLoS Med 2006;3:e270. Atlas Genet Cytogenet Oncol Haematol. 2007;11(1) Cuneo A, Cavazzini F This article should be referenced as such: Cuneo A, Cavazzini F. Myelofibrosis with myeloid metaplasia (MMM), Idiopathic myelofibrosis, Agnogenic myeloid metaplasia. Atlas Genet Cytogenet Oncol Haematol.2007; 11(1):27-29. 29