Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Wernicke–Korsakoff syndrome wikipedia , lookup
Conversion disorder wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Externalizing disorders wikipedia , lookup
Biology of depression wikipedia , lookup
Antidepressant wikipedia , lookup
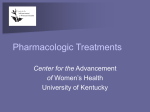
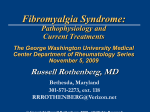
9/30/2013 Boomershine Wellness Centers Personalized Rheumatology Care FIBROMYALGIA 2013 MOVING BEYOND TENDER POINTS Chad S. Boomershine, MD, PhD Medical Director, Boomershine Wellness Centers Medical Director, Elite Healthcare Alliance Assistant Professor of Medicine, Vanderbilt University 330 Mallory Station Road, Suite E‐15 Franklin, TN 37067 Phone 615‐435‐3235 Fax 615‐435‐3275 Chad S. Boomershine, MD, PhD MD and PhD degrees from the Ohio State University Internal Medicine and Rheumatology training at Vanderbilt University. Internationally recognized fibromyalgia (FM) clinician and researcher. Creator of the FIBRO System© for managing FM.1 Author of Medscape Fibromyalgia article 1Boomershine CS. (2010) The FIBRO System: A Rapid Strategy for Management of Fibromyalgia Syndrome. Therapeutic Advances in Musculoskeletal Disease 2(4), 187-200. Disclosure Statement of Financial Interest I, Chad S. Boomerhsine, DO have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation, they are: Affiliation/Financial Interest: Name of Organization (s): Speaker's Bureau: Pfizer, Takeda 1 9/30/2013 Disclosure Statement of Unapproved/Investigative Use I, Chad S. Boomerhsine, DO anticipate discussing the unapproved/investigative use of a commercial product/device during this presentation. Objectives 1. Audience will change the way they diagnose fibromyalgia. 2010 American College of Rheumatology Diagnostic Criteria for Fibromyalgia will be reviewed. 2. Audience will change the way they think of fibromyalgia symptoms. Audience will learn the FIBRO mnemonic for discussing the symptoms of fibromyalgia. 3. Audience will change the way they treat fibromyalgia. CARES mnemonic will be reviewed that outlines the medications used to manage fibromyalgia symptoms. FM Epidemiology • 3.4% of women and 0.5% of men have FM1 – Prevalence increases with age – 80% of people with FM are undiagnosed • Reported female:male ratio 9:1 – True ratio 4:1 female:male – Men have fewer tender points – Men don’t go to the doctor – Providers don’t consider FM in men 1Wolfe F, et al. Arth Rheum 1995;38:19-28 2 9/30/2013 FM Pain Pathogenesis1 BRAIN=PAIN 1) Injury activates peripheral nerves 2) Excitatory signals by peripheral nerves to Inter-neurons = PAIN NMDA-glutamate Norepinephrine (NE) Substance P Serotonin (5-HT) Nitric Oxide GABA and Opioids 3) Inhibitory signals turn off pain and reset the system to baseline 4) Dysregulation of excitatory and inhibitory signals results in FM 1Bennett. FM treatments decrease excitatory signals and increase inhibitory signals to restore balance Mayo Clin. Proc. 1999, 74, 4, 385-98. fMRI Proof: FM Patients have True Pain Gracely RH, et al. Arthritis & Rheum. 2002, 46(5), 1333-1343. 1990 ACR Fibromyalgia Classification Criteria1 Widespread pain ≥3 months: bilateral, above and below waist including spine 2 1 Pain with 4kg/cm2 pressure at ≥11 of 18 Tender points: 1) Occiput- at insertion of suboccipital muscles 2) Trapezius- at midpoint of upper border 3) Supraspinatus- at origins above scapula spine near medial border 4) Gluteal-in upper outer quadrants of buttocks in anterior fold of muscle 5) Greater trochanter- medial and posterior to the trochanteric prominence 6) Low cervical- anterior aspects of intertransverse spaces at C5-7 7) Second rib- second costochondral junction just lateral to the junctions on upper surfaces 8) Lateral epicondyle- 2cm distal to the epicondyles 6 7 3 Back 4 Front 8 5 9 9) Knee- At medial fat pad proximal to the joint line 1Wolfe F, et al. Rheum Dis Clin N Am 1989, 15, 1-18 3 9/30/2013 Classification Criteria miss 1/2 of FM patients1 1990 ACR Classification Criteria 15% Clinical Diagnosis 20% 40% 26% Stop using the ACR Classification Criteria in the clinic.2 1Katz 2J et al., A&R 2006, 54, 1, 169-76. Rheumatol. 2003 Aug;30(8):1671-2 FM is more than just Pain1 FATIGUE FIBROFOG INSOMNIA (Unrefreshed sleep) Depression BLUES Anxiety RIGIDITY (Stiffness) Pain OW! Work difficulty2 OMERACT 9 Hierarcy of domains for fibromyalgia1 1Mease P, et al, J Rheum 2009, 36, 2318-29 2Boomershine CS and Crofford LJ Nature Rev Rheum 2009;5(4):191-9 2010 ACR FM Diagnostic Criteria 4 9/30/2013 FIBRO Diagnosis Simplified PAIN that is Widespread (all body quadrants including spine) and Chronic (at least 3 months) Fatigue both physical and mental (fibrofog) Sleep – wake unrefreshed (still tired) Symptoms must NOT be due to another condition FM Differential Diagnosis/Labs CBC and CMP (anemia, Paget’s, liver/renal disease, diabetes) 25,OH Vitamin D, B12 and folate levels (vitamin deficiencies) Iron, %iron saturation, ferritin (iron deficiency if %sat <20 or ferritin <50) TSH (Thyroid disease) AGE‐APPROPRIATE CANCER SCREENINGS http://www.cancer.org/Healthy/FindCancerEarly/CancerScreeningGuidelines/america n‐cancer‐society‐guidelines‐for‐the‐early‐detection‐of‐cancer ESR and/or CRP (inflammatory disorders‐RA/SLE but also high with obesity) normal ESR is ½ patient age if female, ½ age ‐10 for men Creatinine kinase, LDH, LFTs and aldolase if proximal muscle weakness (inflammatory muscle disease) Hepatitis A/B/C, HIV, Parvo, EBV, Ehrlichia/Borrelia if risk factors FM Differential Diagnosis Psychologic disorders: Major depressive disorder, generalized anxiety disorders, bipolar disease, somatoform disorders Hematologic disorders: Anemia, Leukemia, Lymphoma, Sickle Cell Disease Endocrinologic disorders: Thyroid Disease, Hyperparathyroid Disease, Paget’s Disease, Cushing’s Disease, Diabetes Autoimmune disorders: Polymyalgia Rheumatica, Rheumatoid Arthritis, Systemic Lupus Erythematosis, Sjogren’s Syndrome, Behcet’s Disease, Sarcoid, Vasculitidies Infectious diseases: Human Immunodeficiency Virus, Hepatitis, Parvovirus, Lyme Disease, Epstein Barr Virus, Cytomegalovirus, Urinary Tract Infection Neurologic disorders: Multiple Sclerosis, Myasthenia Gravis, Peripheral Neuropathy Miscellaneous Conditions: Obstructive Sleep Apnea, Periodic Limb Movement Disorder, Restless Legs Syndrome, Cancer, Renal Disease, Vitamin deficiencies (eg, B12, folate, D), Celiac Disease (Sprue), Chiari Malformation, Drug and Alcohol Abuse 5 9/30/2013 Syndromes Associated with FM ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ Interstitial cystitis (bladder pain and inflammation) Migraine headaches Irritable Bowel Syndrome Peripheral neuropathy Low Back Pain and/or Sciatica Chronic Pelvic Pain Chest pain (Costochondritis) Temporomandibular Dysfunction Bursitis – Trochanteric, Shoulder, Knee, Olecranon Tendonitis – biceps, quadriceps, hamstrings EULAR FM Guidelines “Optimal treatment requires a multidisciplinary approach … tailored according to pain intensity, function, associated features, such as depression, fatigue and sleep disturbance …”1 1Ann FATIGUE FIBROFOG INSOMNIA Depression BLUES Anxiety RIGIDITY (Stiffness) Pain OW! Work difficulty2 Rheum Dis. 2008; 67(4) :536-41 2Boomershine CS and Crofford LJ Nature Rev Rheum 2009;5(4):191-9 FIBRO Problem Scale1 0 to 10 scale; 0 = NO PROBLEM and 10 = TOTALLY DISABLING PROBLEM 1. FATIGUE: How much of a problem is FATIGUE or FEELING TIRED? 2. FOG: How much of a problem is THINKING, MEMORY and/or CONCENTRATION? 3. INSOMNIA1: How much of a problem is FALLING ASLEEP? 4. INSOMNIA2: How much of a problem is STAYING ASLEEP? 5. INSOMNIA3: How much of a problem is WAKING UP FEELING REFRESHED? 6. BLUES1: How much of a problem is DEPRESSION or FEELING SAD? 7. BLUES2: How much of a problem is ANXIETY or FEELING NERVOUS? 8. RIGIDITY: How much of a problem is STIFFNESS IN MUSCLES and/or JOINTS? 9. Ow!: How much of a problem is PAIN? 10. GLOBAL: How much of a problem are all your symptoms in total (including any that are not listed above)? 1Boomershine CS. Ther Adv Muscul Dis 2010;2(4):187-200 6 9/30/2013 FM Treatment Algorithm1 1Boomershine CS and Crofford LJ Nature Rev Rheum 2009;5(4):191-9 FM Treatment Algorithm1 1Boomershine CS, et al. Nature Rev Rheum 2009;5:191-9 All FM patients get P.A.I.N.1 • Prescription medications based on problematic symptoms • Activity recommendations: Daily morning stretches along with alternating days of aerobic and resistance exercise 6 days per week. • Information sources: Educate and give handouts and web links: www.fibroguide.com, http://go4life.nia.nih.gov, www.sleepassociation.org • NO Narcotics: Avoid narcotics, benzodiazepines, and steroids – Narcotics have poor efficacy in FM – FM patients can have rebound pain making withdrawal of narcotics difficult – Regulatory issues make prescribing narcotics for fibromyalgia problematic – Tramadol is the only narcotic recommended to treat FM 1Boomershine CS and Crofford LJ Nature Rev Rheum 2009;5(4):191-9 7 9/30/2013 Education and Exercise Recommendations Self-help + Aerobic + Resistance Combination Best1 Daily morning stretches with theraband and low-impact aerobic activity www.fibroguide.com (was www.knowfibro.com) • Comprehensive, individualized, self-directed FM management program • Includes cognitive behavioral modules to reframe negative thinking http://go4life.nia.nih.gov healthy living recommendations for older people 1Rooks DS Arch Intern Med 2007;167:2192–2200 Pharmacotherapy of FM General points: 1) Must rule out and treat disorders that can mimic FM before symptomatic therapies are used. 2) Medications should be started individually at low dose and slowly up-titrated and/or combined - over half of FM patients suffer from multiple medication intolerances.1 Multiple medications or combinations may be necessary, ask patients what medicines worked before. 3) Medications have a limited role in FM treatment, to limit symptoms so patients can participate in non-pharmacologic modalities that provide long-term disease management (exercise, behavioral, and education).2 Nonpharmacologic therapies should be used when possible. 1Slotkoff 2Carville AT et al. (1997) Scand J Rheum 26: 364-7 SF et al. (2008) Ann Rheum Dis 67: 536–541 Limit Polypharmacy • The average FM patient is on 6 medications. • Review medications at first visit. – Get rid of meds that don’t work. – Restart meds that worked before. • Try to find “two-fer” or “three-fer” medicines – One medicine that serves 2 or 3 functions – Amitriptyline at night can help sleep, pain and depression – Gabapentin or pregabalin at night can help sleep and pain and anxiety – Milnacipran in the morning can help pain and fatigue and cognitive dysfunction 1Slotkoff 2Carville AT et al. (1997) Scand J Rheum 26: 364-7 SF et al. (2008) Ann Rheum Dis 67: 536–541 8 9/30/2013 FM Treatment: CARES • CNS pain modulators/anti‐Convulsants • Anti‐depressants/Analgesics/Anti‐spasmotics • Rest (sleep aids, treat OSA and/or RLS) • Exercise/Education (aerobics, resistance, physical therapy, support group, web sites) • Stretching/Stimulants/pSychotherapy Adjuvant Nonopioid Meds for Pain • Anti-Convulsants – 8 carbamazepine*, gabapentin*, pregabalin, topiramate, zonisamide*, ethosuximide, lamotrigene, oxcarbazepine • Anti-Depressants – 12 amitriptyline*, nortriptyline*, fluoxetine*, paroxetine*, buspirone *, desipramine, venlafaxine, desvenlafaxine, duloxetine, milnacipran, velazodone, bupropion • Anti-Inflammatories- 19 meloxicam*, naproxen*, diclofenac*, indomethacin*, ibuprofen*, ketoprofen, flurbiprofen, oxaprozin, ketorolac, etodolac, sulindac, tolmetin, piroxicam, celecoxib, salsalate, diflunisal, choline magnesium trisalicylate, meclofenamate, nabumetone • Muscle Relaxers – 8 baclofen*, cyclobenzaprine*, methocarbamol, orphenadrine, chlorzoxazone, tizanidine*, metaxalone, carisoprodol *Indicates medicines that are on $4/month lists 1Boomershine CS. Pain Medicine News. In Press. FM “Anchor” drugs • Pregabalin (Lyrica)1 – α2δ calcium channel antagonist • Decreases presynaptic excitatory neurotransmitter release (ascending pain pathways) – FDA approved for FM, DPN, PHN, spinal cord injury pain and add-on therapy for seizure disorders – FDA approved FM dosing 150 or 225mg twice daily • Start with 25mg with dinner/evening snack • Up-titrate in weekly intervals as needed/tolerated • AM dose not usually required unless patient has severe allodynia or neuropathic symptoms 1Boomershine CS. Journal of Pain Research, 3, 81-88 9 9/30/2013 Pregabalin: adverse reactions1 Adverse reaction 150 mg/d 300 mg/d 450 mg/d Dizziness 23 31 43 600 mg/d Placebo 45 9 Somnolence 13 18 22 22 4 Weight gain 8 10 10 14 2 Increased appetite 4 3 5 7 1 Peripheral Edema 5 5 6 9 2 Fatigue 5 7 6 8 4 Attention disturbance 4 4 6 6 1 Memory impairment 1 3 4 4 0 Confusional state 0 2 3 4 0 Euphoric Mood 2 5 6 7 0 Vision blurred 8 7 7 12 1 Dry mouth 7 6 9 9 2 Constipation 4 4 7 10 2 http://labeling.pfizer.com/ShowLabeling.aspx?id=561 Pregabalin‐ Warnings and Precautions1 • • • • Angioedema, risk increased with ACE inhibitor use Hypersensitivity reactions can occur Theoretical seizure risk‐ gradually discontinue Antiepileptic drugs, including LYRICA, may increase the risk of suicidal thoughts or behavior. Peripheral edema‐noncardiac, increases with dose Dizziness and Somnolence‐avoid CNS depressants and heavy machinery Weight gain Tumorigenic potential in mice, unknown human risk Ophthalmological effects‐blurred vision Creatinine Kinase Elevations Decreased Platelet Count PR Interval Prolongation • • • • • • • • http://labeling.pfizer.com/ShowLabeling.aspx?id=561 FM “Anchor” drugs • Duloxetine (Cymbalta)1 – Serotonin and Norepinephrine Reuptake Inhibitor • Increases activity of descending anti-nociceptive pathways • “Balanced” 5-HT and NE reuptake inhibition – FDA approved for FM, DPN, Chronic OA Pain, Chronic Low Back Pain, Depression, and Anxiety – Approved dose 60mg once daily • Start 20-30mg with breakfast • Up-titrate monthly if needed and tolerated GENERIC in December 2013 1Sholz BA, et al. Journal of Pain Research 2, 99-108 10 9/30/2013 Duloxetine: adverse reactions1 Adverse Reaction Duloxetine Placebo Nausea 29 11 Decreased appetite 11 2 Dry mouth 18 5 Constipation 15 4 Diarrhea 12 8 Headache 20 12 Fatigue 15 8 Insomnia 16 10 Somnolence 11 3 Agitation 6 2 Dizziness 11 7 Orgasm Abnormal 3 <1 Libido decreased 2 <1 Ejaculation disorder 4 0 Penis disorder 2 0 Hyperhidrosis 7 1 1http://pi.lilly.com/us/cymbalta-pi.pdf Duloxetine: Warnings and Precautions1 – Boxed warning for Suicidality in children and young adults – – – – – – Hepatotoxicity risk – Monitor LFTs and avoid alcohol use Avoid in patients with hepatic insufficiency or CrCl <30 mL/min Blood pressure‐hypertension, hypotension/syncope and tachycardia Serotonin Syndrome/Neuroleptic Malignant Syndrome Abnormal Bleeding Risk Withdrawal symptoms with discontinuation, especially when abrupt – – – – – – – Activation of mania or hypomania‐ recommend bipolar disease screen Caution in patients with history of seizure disorder Avoid Inhibitors of CYP1A2 or Thioridazine Diabetics‐worsening glycemic control and slows gastric emptying Urinary hesitancy and retention Narrow angle glaucoma Hyponatremia especially elderly • dysphoric mood, irritability, agitation, dizziness, sensory disturbances, anxiety, confusion, headache, lethargy, emotional lability, insomnia, hypomania, tinnitus, and seizures 1http://pi.lilly.com/us/cymbalta-pi.pdf FM “Anchor” drugs • Milnacipran (Savella)1 – Norepinephrine and Serotonin Reuptake Inhibitor • Increases activity of descending anti‐nociceptive pathways • 3:1 Norepinephrine:Serotonin reuptake inhibition in vitro – FDA approved for FM management – Anti‐depressant in Europe (1998) and Japan (1999) – Approved dose 50‐100 mg twice daily • Dose‐titration pack ‐ starts with 12.5 mg once daily • SLOWER up‐titration improves tolerability – I give 2 packs, have patient start 1 just in morning and add second dose in evening if tolerate 50mg qam x1 week, takes 1 month 1Ormseth M, et al. Journal of Pain Research 3, 15-18 11 9/30/2013 Milnacipran: adverse reactions Adverse Reaction 100 mg/day 200 mg/day Placebo Nausea 35 39 20 Constipation 16 15 4 Vomiting 6 7 2 Dry Mouth 5 5 2 Headache 19 17 14 Migraine 6 4 3 Dizziness 11 10 6 Hot flush 11 12 2 Palpitations 8 7 2 Heart rate increased 5 6 1 Tachycardia 3 2 1 Hypertension 7 4 2 Blood pressure increased 3 3 1 Hyperhidrosis 8 9 2 1http://frx.com/pi/Savella_pi.pdf Milnacipran: – – – – – – – – – – – – Warnings and Precautions1 Boxed warning for Suicidality in children and young adults Hepatotoxicity risk – Monitor LFTs and avoid alcohol use Blood pressure‐hypertension, hypotension/syncope and tachycardia Serotonin Syndrome/Neuroleptic Malignant Syndrome Abnormal Bleeding Risk Withdrawal symptoms with discontinuation Theoretical risk for activation of mania or hypomania Caution in patients with history of seizure disorder Avoid in patients with substantial alcohol use or chronic liver disease Urinary hesitancy and retention Narrow angle glaucoma Hyponatremia 50% dose ↓ Severe Renal Impairment (CrCl <30 mL/min) 1http://frx.com/pi/Savella_pi.pdf Which to choose? • Direct efficacy comparisons impossible1 – Pregabalin if sleep problems predominate • Limit daytime use if fatigue or cognitive dysfunction severe – Duloxetine if depression or anxiety predominate • Avoid if renal/liver dz; caution in diabetes, migraine, insomnia, IBS – Milnacipran if fatigue or cognitive dysfunction predominate • Avoid in liver disease; caution in IBS, migraine • Combination therapy may be beneficial – Decreased pain with gabapentin‐venlafaxine combination in DPNP patients who failed gabapentin mono‐therapy2 – Pregabalin + milnacipran better in FM patients who failed pregabalin mono‐therapy3 with reduced severity of side effects 1Boomershine 2008 Nat Clin Pract Rheum 12: 636-7 DA 2001 J Clin Neuromuscul Dis 3: 53–62 M, et al. Ann Rheum Dis 2010; 69: 448 2Simpson 3Farmer 12 9/30/2013 NON-FDA Approved Substitutes • Older specific serotonin reuptake inhibitors (SSRIs) have norepinephrine activity and can improve FM symptoms at high doses (fluoxetine 80mg/d)1 – Combine SSRI with an agent that inhibits norepinephrine reuptake such as TCAs (amitriptyline), trazadone, or amoxetine (Strattera) – Amitriptyline 25mg qhs + fluoxetine 20mg qam – Risk for serotonin syndrome when combining serotonin‐active drugs • Amitriptyline provides balanced norepinephrine and serotonin re‐uptake inhibition and has been shown in multiple meta‐ analyses to be effective in FM patients2,3 • Gabapentin mean dose 600mg tid has efficacy in treating FM4 1Am J Med. (2002) 112: 191-7 2Arth Rheum (2008) 59: 1279-98 (2008) 47: 1741-6 Rheum (2007) 56: 1336-44 3Rheum 4Arth Fatigue and Fibrofog • Non‐stimulant wakefulness promoting agents – Modafinil (Provigil) • FDA‐approved for obstructive sleep apnea (OSA), narcolepsy, and shift‐work‐syndrome • 3 reports supporting use in treating FM fatigue1,2,3 – Doses ranged from 50‐400mg daily given as a single am dose or divided morning and noon – ?Armodafinil (Nuvigil) active enantiomer of modafinil • Stimulants‐ methylphenidate (Ritalin), dexmethylphenidate (Focalin), amphetamines (Adderall) – Methylphenidate 5‐10mg qam and noon • SR preparation allows once daily dosing 1J Clin Rheum (2007) 13: 52 Clin Rheum (2003) 9: 282-5 3J Neuropsych Clin Neurosci (2001) 13: 530-1 2J Insomnia Evaluation • Identify specific sleep problem • Restless legs syndrome(RLS), obstructive sleep apnea(OSA) – RLS in 1/3 of FM patients, screen using RLS Study Group criteria1 • Have you ever experienced a disagreeable feeling in the legs, with aching, creeping, and motor restlessness, with an urge to move the legs? If answer YES, ask: – Do these symptoms appear mainly when sitting or lying down? – Are these symptoms worse at night? – Is any relief of these symptoms obtained by leg movement or walking? Patient Berlin Questionnaire criteria2 should have formal sleep study • Persistent snoring and daytime somnolence and hypertension or obesity predicts OSA with 86% sensitivity and 77% specificity2 • Epworth Sleepiness Scale is very poor at identifying OSA 1Movement 2Ann Disorders (1995) 10: 634-42 Intern Med (1999) 131: 485-91 13 9/30/2013 Insomnia Treatments • Benzodiazepines should be avoided in FM patients • Sedating antidepressants can benefit depressed patients • Ramelteon (Rozerem) and eszopiclone (Lunesta) are recommended FDA approved therapies for insomnia, zolpidem (Ambien) 2nd line – Ramelteon is a selective melatonin receptor agonist given as 8mg tablet 90 minutes before bedtime followed by a hot shower • Usually well tolerate, no sedation, no “hang‐over” the next day – Eszopiclone is a nonbenzodiazepine hypnotic given as a 1, 2 or 3mg tablet immediately before bedtime • Patients should be monitored for worsening depression or suicidal ideation • Use with other sedatives should be avoided – Headache and dysgeusia (unpleasant taste sensation) can limit tolerability Zolpidem dosing 50% maximum in women due to sedation risk • Sodium Oxybate (Xyrem or GHB) – Improves sleep and global FM symptoms1 – Indication rejected due to safety concerns 1Russell IJ, et al. Arthritis Rheum. 2009;60:299-309 Sedating Antidepressants • Tricyclic antidepressants (TCAs): amitriptyline, desipramine, nortriptyline, and cyclobenzaprine – Low evening doses (5‐10mg cyclobenzaprine, 10‐50mg amitriptyline) – Intolerance to higher doses often makes TCA monotherapy insufficient to manage FM or mood disorders – Combining low‐dose TCAs with fluoxetine 20mg daily can provide synergy for treating FM symptoms with minimal side effects1 • Mirtazapine (Remeron) enhances serotonergic and noradrenergic neurotransmission via a novel mechanism – May allow use in patients who do not tolerate traditional SNRIs – 15‐30mg at night improves FM pain, insomnia, fatigue, depression2 – Somnolence inversely proportional to dose, increase if too sedating • Trazodone is the most sedating antidepressant – 100mg qhs improves sleep architecture3 1J Clin Psychiat (2008) 69 (suppl 2): 25-30 2Pharmacopsychiatry 3Neuropsychobiol (2005) 37: 168-70 51: 148-63 RLS Management • Replete Iron stores – Ferritin should be ≥50ug/L (100 optimal), %iron saturation ≥20%1 • If inflammation present, divide ferritin by 3 to get true value • soluble transferrin receptor (mg/L)/ferritin (mcg/L) ratio – If <1 likely anemia of chronic disease, if >2 likely iron deficiency anemia • Dopamine agonists – Pramipexole (Mirapex) and ropinirole (Requip) approved for RLS – Both have demonstrated efficacy in managing FM2,3 – Start at low dose (0.125mg for pramipexole and 0.25mg for ropinirole) 2 hours before bedtime – Increased in weekly intervals until RLS symptoms resolve or patients become intolerant • Recommended maximum doses for RLS: pramipexole 0.5mg and ropinirole 4mg • Higher doses for FM symptoms (mean 4.5mg for pramipexole and 6mg for ropinirole) – Generic carbidopa/levodopa (25 and 100mg, respectively) combination tablets can be used to treat RLS off‐label 1Sleep 2Arth 3J Med Reviews (2001) 5: 277-86 Rheum (2005) 52: 2495-505 Clin Rheum (2003) 9: 277-9 14 9/30/2013 Antidepressants • FM patients often have major depressive disorder (30%) or an anxiety disorder (40%) • Duloxetine is recommended first‐line treatment – Milnacipran monotherapy doesn’t work well for depression in FM • Desvenlafaxine (Pristiq) generic SNRI, similar to Cymbalta • Venlafaxine (Effexor) is generic SNRI shown to improve FM symptoms at dose of 75mg once daily1 • Older selective serotonin reuptake inhibitors (SSRIs): fluoxetine (Prozac) and paroxetine (Paxil) – Inhibit norepinephrine reuptake at 40‐80mg per day – High doses often poorly tolerated SNRIs should be gradually tapered as rebound increases in depression and withdrawal symptoms may occur 1Sayar et al. Ann Pharmacother 2003;37(11):1561-5 Stiffness Treatments • Daily morning stretching • Cyclobenzaprine (Flexeril) – A tricyclic antidepressant (TCA) – Significantly improves global FM symptoms along with pain, sleep, and tender points1 – 30‐50mg divided over the day can manage FM “flares” • Dose typically limited by sedation • Nightly 15 or 30mg extended release (Amrix) is less sedating2 – Monitor for worsening fatigue and anticholinergic side effects (dry mouth, urinary retention, etc.) – Avoid use with other CNS depressants 1Arth Rheum (2004) 51: 9-13 2http://www.amrix.com/pdf/AMR-001b_072808_Blueline.pdf Stiffness Treatments • Tizanidine (Zanaflex) is central α2‐adrenergic agonist – Start with 4mg qhs, maximum dose of 36mg divided over the day – Along with anticholinergic side effects, tizanidine can cause hepatotoxicity and laboratory monitoring is strongly recommended • Methocarbamol (Robaxin) and metaxalone (Skelaxin) – Less sedating, limited published evidence in managing FM • Antispastics (baclofen and dantrolene) can be helpful especially in FM patients with muscle cramps • Benzodiazepines should be avoided in FM patients due to addiction potential and worsening of nonrestorative sleep. • Tramadol can significantly improve FM stiffness and will be discussed in the next section. 15 9/30/2013 Analgesics • Acetaminophen (APAP) has proven efficacy in FM – Treatment failures are common since required dosing is near 4000mg/day and usually divided 6‐8 times per day – Compliance can be improved using extended‐release formulations of 1000mg four‐times daily – Known APAP hepatotoxicity‐ lab monitoring required • Most patients prefer NSAIDs over APAP1 – Evidence for efficacy of NSAIDs in FM is lacking – NSAIDs are not recommended in the absence of a concomitant inflammatory condition or OA/bursitis that can serve as a pain generator in FM 1Arth Rheum (2001) 44: 2451-5 Tramadol (Ultram) • Traditional narcotics should be avoided in FM treatment – Poor Efficacy and can cause Rebound Pain • Tramadol is a narcotic combining mu‐opioid agonist and SNRI activities recommended for managing FM1 – One or two tramadol/acetaminophen 37.5/325mg tablets taken 4 times daily can significantly improve pain, stiffness and work interference in FM patients2 – Side effects include nausea, pruritis and constipation – Risk of abuse and dependence is low • 97% of cases occur in patients with a prior history of substance abuse3 • Recommend screening for prior substance abuse before prescribing • Tapentadol (Nucynta) – Weak mu‐opioid agonist with NRI activity – Acute pain indication only 1Ann 2Arth Rheum Dis (2008) 67: 536–541 Rheum (2005) 53: 519-27 Alcohol Depend (1999) 57: 7-22 3Drug Conclusions • FM patients can be very rewarding to treat • Identify and treat disorders that can mimic FM • Pharmacologic therapies work best when combined with nonpharmacologic treatments • The FIBRO mnemonic with the FIBRO Problem and Change Scales provide a rapid, symptom‐ based method for assessment and management of FM patients designed for use in busy clinics 16 9/30/2013 Boomershine Wellness Centers Personalized Rheumatology Care FIBROMYALGIA 2013 MOVING BEYOND TENDER POINTS Chad S. Boomershine, MD, PhD Medical Director, Boomershine Wellness Centers Medical Director, Elite Healthcare Alliance Assistant Professor of Medicine, Vanderbilt University 330 Mallory Station Road, Suite E‐15 Franklin, TN 37067 Phone 615‐435‐3235 Fax 615‐435‐3275 17