Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
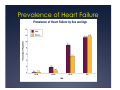
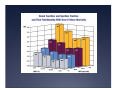
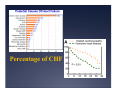
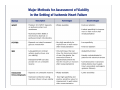
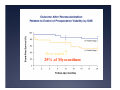
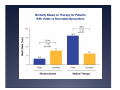
Heart Failure Facts 5.7 million in US with 670 k per year newly diagnosed Increases with age from 40-80 (male>female) Lifetime risk of 1 in 5: 1 in 9 in men and 1 in 6 in women if no MI Definition of Heart Failure Classification Ejection Fraction Description I. Heart Failure with Reduced Ejection Fraction (HFrEF) ≤40% Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFrEF and it is only in these patients that efficacious therapies have been demonstrated to date. II. Heart Failure with Preserved Ejection Fraction (HFpEF) ≥50% Also referred to as diastolic HF. Several different criteria have been used to further define HFpEF. The diagnosis of HFpEF is challenging because it is largely one of excluding other potential noncardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified. a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFpEF. b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF previously had HFrEF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients. DEFINTION OF CHF HF is the clinical syndrome that results from structural or functional abnormalities that impair the ability of the heart to fill with or eject blood. All forms of cardiac disease can lead to heart failure with reduced ejection fraction (HFREF). Myocardial pressure overload, volume overload, or decreased contractility trigger adaptive responses whose purpose is to improve cardiac output and maintain blood flow to vital organs. These responses become persistent, and lead to the structural and molecular changes that characterize ventricular remodeling. HFREF typically progresses gradually from asymptomatic LV systolic dysfunction to a symptomatic state characterized by dyspnea, fatigue, and volume overload. Definition of Heart Failure Elements of the Heart Failure Process Hemodynamic Chamber remodeling Compositional Remodeling Neurohormonal Prevalence of Heart Failure Gender 1/3rd less in women but still 50% due to longer life expectancy Incidence of CAD lower in women but effect on CHF greater Hypertension, valvular heart disease, obesity, and diabetes mellitus are more powerful predictors of HF risk in women than in men Mortality ICM>NICM 10 year 20% survival if symptoms Median male=1.7 years Median female: 3.2 years Greater in African Americans Risk Prediction: Seattle Heart Failure Model Risk Predictor Advanced NYHA Class Ischemic High diuretic dose Low EF Low BP Hyponatremia Low Hemoglobin Increase Uric Acid Decreased Cholesterol 77 year old female History of hypertension, diabetes mellitus, and hyperlipidemia. She has had progressively reduced exercise tolerance over the past 2 years. She denied any orthopnea, PND, or leg edema. Over the past month, her exercise tolerance has been reduced to ½ block with mild ankle edema and mild orthopnea. Last evening she awoke breathless with chest pressure, and was rushed to the ER. BP=210/110, pulse=120 RR=32 (BP:160/100 p=98 with 2 doses of Lasix) JVP 6cm H20, carotid upstrokes normal Lungs: crackles diffusely Cor: PMI 5ICS 1 cm left MCL, S4, 1/6 SEM 2nd RICS Abd: liver 1 cm below RCM, Extr: 1+ edema Labs Hb 13.2, Hct=42% K 4.2, HCO3 24, BUN 29, Cr 1.6, Glu 161 Chol 223, TG 250, LDL 151 CPK 83, Troponin T <0.01 Which of the following risk factors in this patient would predict increased mortality? Reduced hemoglobin Chronic renal insufficiency Acuteness of presentation Normal LV ejection fraction QRS duration Which of the following risk factors in this patient would predict increased mortality? Reduced hemoglobin Chronic renal insufficiency Acuteness of presentation Normal LV ejection fraction QRS duration Symptoms and Signs in CHF Congestion-Volume overload Dyspnea: Exertional dyspnea is likely due to an augmented ventilatory response to exercise, inefficient gas exchange due to ventilation/perfusion mismatch, and skeletal muscle alterations that trigger increased ventilatory drive. Tissue edema: ascites, edema, early satiety PE: crackles present in only 15% due to increased lymphatic drainage. JVP more useful as physical signs Symptoms and Signs in CHF Low output/Poor Perfusion Nausea, abdominal pain, fatigue Diminished peripheral pulses, cool extremities, pallor, peripheral cyanosis Pulsus alternans While low blood pressure is common, a proportional pulse pressure (PPP = [systolic blood pressure -diastolic blood pressure]/systolic blood pressure) of <25% can often predict a cardiac index of <2.2 L/min on right heart catheterization Resting sinus tachycardia may be a compensatory response to very low stroke volume 71 year old female She was s/p CABG for left main and 3 vessel disease She did well for several years and presented with chest pain and dyspnea. She also noted mild leg swelling. PE: BP 90/52, p=118/min, RR=24/m Frail elderly female mildly dynpneic JVP up to angle of the jaw and +HJR, low volume carotids PMI 5 ICS 2 cm lateral to the MCL with S3 and MR murmur Liver 1 cm below RCM 1+ edema Which of her physical exam findings has the highest likelihood of support a diagnosis of heart failure? Elevated JVP Edema Any murmur S3 Edema Which of her physical exam findings has the highest likelihood of support a diagnosis of heart failure? Elevated JVP Edema Any murmur S3 Edema Imaging in CHF CXR: cardiac size, congestion, alternative diagnoses Echocardiography: Imaging in CHF Cardiac MR: Chamber size Chamber function Valve disease Gadolinium uptake-scar Specific diagnoses-amyloid etc Coronary disease-proximal Imaging In Heart Failure Electrocardiography (ECG Evidence of previous MI suggests an ischemic cause, Rapid heart rate may raise suspicion for tachycardiamediated cardiomyopathy. Low voltage on ECG in a patient with left ventricular dysfunction and may suggest an infiltrative cardiomyopathy. ECG may also be used to assess for arrhythmias or electrical dyssynchrony (prolonged QRS interval) if cardiac resynchronization therapy is being considered and to monitor the QT interval during treatment with specific medications. Radiography is inaccurate for measuring cardiac chamber enlargement, which should be assessed with echocardiography; Absence of overt pulmonary edema on CXR does not preclude elevated intracardiac filling pressures, particularly in patients with long-standing heart failure, likely owing to increased efficiency of mediastinal lymphatic drainage. Lab Evaluation Focus on end organ dysfunction Renal Liver Cardiac enzymes in ACS is also present Etiologies of heart failure (thyroid, immunoglobulin etc) Na Hb BNP Diagnostic if >100 Prognostic: Elevated levels are associated with worse prognosis across the spectrum of heart failure severity and provide further prognostic information in addition to peak exercise oxygen consumption and ejection fraction (EF) for predicting death Decompensated heart failure, a discharge BNP <300- reduced readmits Troponins Elevations in cardiac troponins (T, I) may also be observed in the setting of decompensation and in stable heart failure. The degree of troponin elevation depends on the underlying disease, The presence/absence of acute coronary syndromes, Acuity of presentation. Such elevations occur in as many as 23% of patients with stable chronic heart failure and in as many as 55% of ADHF patients These elevations are associated with lower EF, worse prognosis, and more severe symptoms. Elevated troponin T was an independent predictor of death (3.4 times higher risk of mortality). 71 year old female She was s/p CABG for left main and 3 vessel disease She did well for several years and presented with chest pain and dyspnea. She also noted mild leg swelling. PE: BP 90/52, p=118/min, RR=24/m Frail elderly female mildly dyspneic JVP up to angle of the jaw and +HJR, low volume carotid PMI 5 ICS 2 cm lateral to the MCL with S3 and MR Liver 1 cm below RCM 1+ edema What elements of the history, physical exam, and CXR suggests heart failure? Elevated JVP, BP, carotid upstrokes, and respiratory rate Cardiomegaly, edema, liver size, and MR murmur Elevated JVP, heart rate, S3, and dyspnea at rest Respiratory rate, liver size, edema, and pleural effusion What elements of the history, physical exam, and CXR suggests heart failure? Elevated JVP, BP, carotid upstrokes, and respiratory rate Cardiomegaly, edema, liver size, and MR murmur Elevated JVP, heart rate, S3, and dyspnea at rest Respiratory rate, liver size, edema, and pleural effusion CAD and CHF Risk post MI (RR)=6 vs 2.5 for HBP PAR=50% for hypertension and 25% for MI CAD as cause of CHF MI Ischemia, including stunning and hibernation Endothelial dysfunction; Mitral regurgitation, especially after inferior MI’s. 67 Year Old Female Long history of 1-2 blocks of DOE Recently, her legs began swelling and she needed pillows at night to be comfortable Tonite, she awoke acutely SOB Hx HBP, DM, 1ppd smoker PHYSICAL EXAM BP 180/120, p 98, RR=32 JVP 6 cm H2O Chest: diffuse crackles and decreased breath sounds at right base Cor: PMI slightly displaced; 1/6 basal ejection murmur and S4 Abd: liver RCM Extr: intact pulses and 1+ edema LABS Hb=15.1 gm K 4.2, BUN 29; Cr 1.4 CPK 41, troponin 0.08 PO2=61 on room air ECHO EDD=5.6 cm; ESD=4.4 cm EF=38% LA=4.5 cm PWTd=1.3 cm Doppler: E/A reversal, deceleration time =160 msec, mild MR, mild TR with 3.2 m/s Following stabilization, What would your 1st course of action be? Uptitration of beta blocker using carvedilol Begin ARB and titrate upwards to full dose CTA to assess more accurately LV systolic function for ICD consideration Coronary angiography for consideration of revascularization Beta blocker and ACEI therapy as patient has had a previous MI Following stabilization, What would your 1st course of action be? Uptitration of beta blocker using carvedilol Begin ARB and titrate upwards to full dose CTA to assess more accurately LV systolic function for ICD consideration Coronary angiography for consideration of revascularization Beta blocker and ACEI therapy as patient has had a previous MI Percentage of CHF Cases VIABLE MYOCARDIUM Myocardium that is alive is viable Viable myocardium will contract when stimulated and if sufficient blood flow Viable myocardium subserved by a stenotic coronary vessel or has impaired coronary flow reserve is at risk for infarction The more myocardium at risk and the worse the LV function, the higher the event rate How much? 25% of Myocardium VALUE OF REVASCULARIZATION May increase EF Avoid further ischemia Reduce sudden death Avoid remodeling even if no EF change or improvement in wall motion Epicardium may contract preventing further expansion Reverse remodeling and decrease LV size if wall motion and thickening improve Aspirin and Statins in CAD and CHF Meta-analysis: ACE inhibitor trials involving patients with ischemic HF. With aspirin therapy, there is a statistically smaller magnitude of benefit of ACE inhibitors for reduction in total mortality and MIs. In Warfarin versus aspirin in HF trials, aspirin was associated with increased rates of HF admissions. Statins do not appear to provide incremental benefits when added to standard HF medications. The large-scale randomized CORONA trial showed no significant reduction in the primary outcomes of CV death, nonfatal MI, and nonfatal stroke. Most deaths were sudden death (43%) or progressive HF (26%). Very few were due to fatal MIs (only 2%). ACEI ACE inhibitors were the first agents shown to reduce the rate of progression of LV remodeling, by diminishing or preventing the progressive LV dilation observed in patients following large MI’s SAVE CONSENSUS SOLVD-RX and Prevention ACEI Principal adverse effects of renal impairment, hypotension, and hyperkalemia are mediated by withdrawal of angiotensin II effects on the renal glomerular efferent arteriole (with resulting reduction in glomerular filtration pressure), the peripheral arterial bed, and the zona glomerulosa of the adrenal gland. Cough is from bradykinin not being broken down Angioedema Use of ARB should be reserved primarily for cough. Angioedema is rarely caused by ARB 62 year old male Patient is s/p MI 2 years ago with increasing dyspnea on exertion. He has history of hypertension and smoking. PE: 124/68, p=86, RR=18 JVP 9 cm H20 and +HJR and normal carotids Chest: bilateral basilar crackles Cor: displaced PMI S4 1/6 SEM Abdomen: Liver and spleen normal Extr: no edema. EKG: SR old ASMI MPI: anterior hypoperfusion at stress and rest in anterior and septal walls: EF=34% and LV dilatation Labs: Hb=14, Cr=2; BUN=39 Which of the following approaches will reduce his symptoms? Furosemide 40-80 mg/day Bumex 2 mg daily Na restriction and 20 mg Lasix Dig 0.125 md/day and furosemide 20 mg, and Na restriction All of the above Which of the following approaches will reduce his symptoms? Furosemide 40-80 mg/day Bumex 2 mg daily Na restriction and 20 mg Lasix Dig 0.125 md/day and furosemide 20 mg, and Na restriction All of the above ARB’s and ACEI’s Modest elevation in serum creatinine usually represents a pharmacologic hemodynamic effect of the drug, related to renal efferent arteriolar dilation, and not renal injury. Such a modest elevation should not necessarily trigger drug discontinuation or even dose reduction. Which of the following regimens will reduce symptoms, prolong survival and reduce CHF hospitalizations? Furosemide 40 mg/day Captopril 6.25 mg/day Na restriction and 20 mg Lasix Dig 0.125 md/day and furosemide 20 mg, and Na restriction Lisinopril 20-40 mg/day Which of the following regimens will reduce symptoms, prolong survival and reduce CHF hospitalizations? Furosemide 40 mg/day Captopril 6.25 mg/day Na restriction and 20 mg Lasix Dig 0.125 md/day and furosemide 20 mg, and Na restriction Lisinopril 20-40 mg/day ARB’s HEAAL (Heart Failure Endpoint Evaluation of AIIAntagonist Losartan) trial demonstrated the superiority of losartan 150 mg daily over losartan 50 mg daily on the composite primary endpoint of death or HF hospitalization in patients with HF, reduced LVEF, and prior ACEI intolerance. Demonstrated a dose response for outcome effects of ARBs Documented the incremental clinical value of incremental renin-angiotensin aldosterone system inhibition, Substantiated that drugs should be prescribed with the dosing strategy associated with clinical trial results 62 year old male Patient is s/p MI 2 years ago with increasing dyspnea on exertion. He has history of hypertension and smoking. PE: 124/68, p=86, RR=18 JVP 5 cm H20 and -HJR and normal carotids Chest: bilateral basilar crackles Cor: displaced PMI S4 1/6 SEM Abdomen: Liver and spleen normal Extr: no edema. EKG: SR old ASMI MPI: anterior and septal hypoperfusion at stress : EF=34% and LV dilatation On furosemide 40 mg and started on Lisinopril 20 mg/d for 2 weeks returns with a cough and now her BUN=45; creatinine is 2.3 ;Labs were Hb=14, Cr=2; BUN=39 What might your next course of action be? Stop the Lisinopril and use hydralazine 10 mg HS Stop the lisinopril and start Losartan 50 mg because Cr has increased to 2.3 Stop the lisinopril and start Losartan 50 mg for cough; the creatinine is increased <25% is of limited concern Add Losartan 50 mg rather than increasing lisinopril due to the cough Can not use lisinopril-will have to use a beta blocker only due to the rise in creatinine What might your next course of action be? Stop the Lisinopril and use hydralazine 10 mg HS Stop the lisinopril and start Losartan 50 mg because Cr has increased to 2.3 Stop the lisinopril and start Losartan 50 mg for cough; the creatinine is increased <25% is of limited concern Add Losartan 50 mg rather than increasing lisinopril due to the cough Can not use lisinoptil-will have to use a beta blocker only due to the rise in creatinine Beta Blockers Beta-blocker effects include: Reduced heart rate, Beta-receptor up-regulation and improved coupling to intracellular signaling pathways Altered myocardial metabolism, Improved calcium transport, Inhibit renin-angiotensin system inhibition Inhibition of endothelin and inflammatory cytokine secretion. Beta-blockers reduce and reverse LV remodeling. Dose-related and progressive over time Improvement in LVEF was observed with incremental carvedilol doses between 6.25 mg and 25 mg twice daily. Beta Blockers Guideline recommend beta-blockers for symptomatic and asymptomatic patients with HF and LVEF ≤40%, For hospitalized patients, the recommendation is to initiate treatment in-hospital once volume status is optimized and intravenous vasoactive/inotropic agents are discontinued. Treatment should be initiated at low doses, with uptitration generally at 2-week interval with maintenance of therapy at the maximal tolerated dose. In the presence of worsening symptoms as outpatient, adjust the dose of diuretics and other vasoactive agents. Alternatively, the titration interval may be prolonged and/or the target dose may be reduced. Wherever possible, beta-blockers should be continued, possibly with a dose reduction, in the setting of an HF exacerbation. Abrupt discontinuation should be avoided. 62 year old male Patient is s/p MI 2 years ago with increasing dyspnea on exertion. He has history of hypertension and smoking. PE: 124/68, p=86, RR=18 JVP 9 cm H20 and +HJR and normal carotids Chest: bilateral basilar crackles Cor: displaced PMI S4 1/6 SEM Abdomen: Liver and spleen normal Extr: 2+ edema. EKG: SR old ASMI Started on Lisinopril 20 mg/d for 2 weeks with furosemide 40 mg and begun on Carvedilol 12.5 mg BID and returns dyspneic in one week. Chest crackles at bases and no wheezing. Cr is now 2.2 and was 2.0 Why did the patient develop dyspnea? Need to start at maximal dose as patient decompensated prior to beta blocker dosing Titration should begin in decompensated patients at 3.125 mg BID-received too high of a dose and should be better diuresed Digoxin was not started to prevent decompensation with beta blocker use Patients should be overdiuresed before beginning beta blockers Creatinine was too high for a beta blocker and now have toxicity Why did the patient develop dyspnea? Need to start at maximal dose as patient decompensated prior to beta blocker dosing Titration should begin in decompensated patients at 3.125 mg BID-received too high of a dose and should be better diuresed Digoxin was not started to precvent decompensation with beta blocker use Patients should be overdiuresed before beginning beta blockers Creatinine was too high for a beta blocker and now have toxicity Starting ACEI/ARB’s and Beta Blockers ACEI/ARB’s-start low and avoid hypotension Beta Blockers-start when euvolemic Starting simultaneous? Will land up with lower doses than are optimal Maximizing beta blocker is more important Suggest: low dose ACEI to get started and titrate up the beta blocker Aldosterone Inhibition Aldosterone is secreted by the adrenal cortex and other tissues, including the heart and vasculature, with release stimulated by angiotensin II, ACTH, and potassium. Its actions include promotion of sodium retention and potassium and magnesium wasting, Induction of myocardial and vascular fibrosis, Activation of the sympathetic nervous system, and inhibition of the parasympathetic system. Circulating levels of aldosterone are markedly increased in patients with HF. ACE inhibition and angiotensin-receptor blockade diminish, but do not abolish, aldosterone secretion, which tends to "escape" over time following institution of reninangiotensin system inhibition. Aldosterone Inhibition RALES: Reduced mortality in Class III CHF with only 10% on beta blockers EPHESUS 13-15% reduction in mortality post MI with 90% on beta blockers EMPHASIS Class II CHF-reduced death and hospitalization 37% (mortality 24%) with >90% on ACEI/ARB and 87% on beta blockers Aldosterone Inhibition Cautions K >5.0 mmol Cr >2.5 Diabetes Concomitant inhibitors of CYP3A4 (eplerenone) 62 year old male Patient is s/p MI 2 years ago with increasing dyspnea on exertion. He has history of hypertension and smoking. PE: 124/68, p=86, RR=18 JVP 6 cm H20 and -HJR and normal carotids Chest: bilateral basilar crackles Cor: displaced PMI S4 1/6 SEM Abdomen: Liver and spleen normal Extr: no edema. EKG: SR old ASMI Started on Lisinopril 20 mg/d and furosemide 40 mg for 2 weeks and begun on Carvedilol 3.125 mg BID and titrated to 12.5 mg BID. He returns dyspneic and fatigued following last titration without any additional improvement. Chest few crackles at bases and no wheezing. Cr is now 2.2 and was 2.0. His K=4.9. His exercise tolerance is still <1 block What would be reasonable additional therapy that would reduce symptoms and have mortality benefit? Increase diuretics to furosemide 80-120/d Add Losartan at 50 mg Use Lisinopril at BID doasages Add Digoxin at 0.25 mg/s Begin to titrate sprironolactopne at 12.5 mg/daily What would be reasonable additional therapy that would reduce symptoms and have mortality benefit? Increase diuretics to furosemide 80-120/d Add Losartan at 50 mg Use Lisinopril at BID doasages Add Digoxin at 0.25 mg/s Begin to titrate sprironolactone at 12.5 mg/daily Hydralazine-Isosorbide Dinitrate VHEFT I-modeeate effect: 43% reduction compared yo placebo Better response in African Americans VHEFT 2-enalapril superior AHEFT: Add on trial with Hydralazine 75-Isordil 40 mg TID for Class III CHF 87%/75%/40% used with ACEI/ARB, BB, Aldo antagonist 43% reduction in mortality 47/25% side effects: headache and dizziness 68% reached target dose 62 year old male Patient is s/p MI 2 years ago with increasing dyspnea on exertion. He has history of hypertension and smoking. PE: 124/68, p=86, RR=18 JVP 6 cm H20 and -HJR and normal carotids Chest: bilateral basilar crackles Cor: displaced PMI S4 1/6 SEM Abdomen: Liver and spleen normal Extr: no edema. EKG: SR old ASMI Started on Lisinopril 20 mg/d and furosemide 40 mg for 2 weeks and begun on Carvedilol 3.125 mg BID and titrated to 12.5 mg BID. He returns dyspneic and fatigued following last titration without any additional improvement. Chest few crackles at bases and no wheezing. Cr is now 2.2 and was 2.0. His K=4.9. His exercise tolerance is still <1 block Would the use of Hydralazine-Isordil be helpful in this patient? Yes- as an add on to any patient fully dosed on ACEI/ARB, beta blocker, and aldosterone antagonist No-BP is too low and is should be restricted to patients with poor BP control Possibly-better to just use the isordil for dyspnea effect Yes-prolongs life, can be added to all of the above therapies but most useful in African Americans No-Too many meds will confuse patient. We should only use 2 + diuretic Would the use of Hydralazine-Isordil be helpful in this patient? Yes- as an add on to any patient fully dosed on ACEI/ARB, beta blocker, and aldosterone antagonist No-BP is too low and is should be restricted to patients with poor BP control Possibly-better to just use the isordil for dyspnea effect Yes-prolongs life, can be added to all of the above therapies but most useful in African-Americans No-Too many meds will confuse patient. We should only use 2 + diuretic Polypharmacy ACEI+Beta Blocker+Diuretic: The specific addition should be influenced by renal function, potassium concentration, blood pressure, and volume status. Choices for additive therapy include: Aldosterone-receptor blocker ARB, Hydralazine/ISDN It should additionally be noted that 40% of the A-HeFT study population was receiving background aldosterone-receptor blockers, providing some evidence for the combination of ACE inhibitors, aldosteronereceptor blockers, and hydralazine/ISDN Digoxin Digoxin Inhibits Na-K ATPase Mild inotrope and improves baroreceptor function Reduces HF hospitalizations perhaps even with EF>45% Mortality neutral if Dig level < 0.8 Diuretics No trial evidence Torsemide better bioavailability Loop diuretics require a threshold urinary concentration before any diuresis is initiated with sigmoid shaped relationship between urinary concentration and fractionl sodium excretion. The latter reaches a concentration plateau. Diuretic Resistance Causes Inadequate diuretic dose Excess sodium intake Reduced diuretic absorption Impaired diuretic urinary excretion (due to chronic kidney disease, advanced age, or CHF), and Concomitant medications Treatment approaches include increased dose, dividing into multiple daily doses, switching from furosemide to torsemide, and adding a thiazide diuretic Heart Failure and Preserved Ejection Fraction Clinical CHF with Normal EF Abnormal diastolic indices Incidence: nearly 50% especially in older patients 60% of women >65 have diastolic CHF 30% of men >65 years old have diastolic CHF Mortality: Higher for HFREF but >50% of the risk of HFREF Morbidity: Reduced exercise tolerance, increased hospitalizations Determination of CHF with Normal EF CHF scales: Boston, Framingham Point score systems that integrate clinical, PE and X-ray findings Overt CHF on admission: rales, pulmonary congestion and normal EF Echo will indicate abnormal relaxation and elevated LV filling pressures DIASTOLIC INDICES Indices suggesting reduced relaxation Prolonged Isovolumic Relaxation Time E/A reversal and prolonged deceleration time Reduced rapid filling mitral annular velocity Indices suggesting elevated LV filling pressures PVI Mitral and pulmonary “A” waves E/Vp E/e’ (Mitral annular Tissue Doppler) Etiologies of Heart Failure and Preserved EF Infiltrative disease Restrictive Cardiomyopathy Hypertrophic Cardiomyopathy Valvular Heart Disease Pericardial Disease HTCVD Diabetes CAD???-ischemia??? HFPEF and Co-Morbidities Management of Heart Failure and Preserved EF Address the co-morbidities: HBP, DM, chronic renal insufficiency, anemia Adequate diastolic filling period: rate control Address volume overload Improve relaxation?? Address remodeling issues: LVH and fibrous tissue content and composition POTENTIAL THERAPEUTIC AGENTS Diuretics Relaxation: beta blockers, calcium channel blockers Hypertrophy: ACEI, ARB’s, Calcium channel blockers, beta blockers Fibrosis: Aldosterone antagonists; ACEI’s Summary of HFPEF Trials Seniors-beta blocker; PEP=ACEI ALDOSTERONE HYPOTHESIS Improved survival and CHF in RALES associated with decreased myocardial collagen content Hyperaldosteronism: greatest LVH, most fibrosis, symptomatic Improved survival and symptoms post MI with antialdosterone therapy (Pitt et al) Spironolactone in HFPEF (TOPCAT) Treatment of HFpEF Recommendations Systolic and diastolic blood pressure should be controlled according to published clinical practice guidelines Diuretics should be used for relief of symptoms due to volume overload Coronary revascularization for patients with CAD in whom angina or demonstrable myocardial ischemia is present despite GDMT Management of AF according to published clinical practice guidelines for HFpEF to improve symptomatic HF Use of beta-blocking agents, ACE inhibitors, and ARBs for hypertension in HFpEF ARBs might be considered to decrease hospitalizations in HFpEF Nutritional supplementation is not recommended in HFpEF COR LOE I B I C IIa C IIa C IIa C IIb B III: No Benefit C 77 year old female History of hypertension, diabetes mellitus, and hyperlipidemia. She has had progressively reduced exercise tolerance over the past 2 years. She denied any orthopnea, PND, or leg edema. Over the past month, her exercise tolerance has been reduced to ½ block with mild ankle edema and mild orthopnea. Last evening she awoke breathless with chest pressure, and was rushed to the ER. BP=210/110, pulse=120 RR=32 (BP:160/100 p=98 with 2 doses of Lasix) JVP 6cm H20, carotid upstrokes normal Lungs: crackles diffusely Cor: PMI 5ICS 1 cm left MCL, S4, 1/6 SEM 2nd RICS Abd: liver 1 cm below RCM, Extr: 1+ edema Labs Hb 13.2, Hct=42% K 4.2, HCO3 24, BUN 29, Cr 1.6, Glu 161 Chol 223, TG 250, LDL 151 CPK 83, Troponin T <0.01 What specific therapies are ther available to prolong life in this patient? ARB/ACEI Beta blockers Spironolactone if you live in Canada Control BP None of the above What specific therapies are there available to prolong life in this patient? ARB/ACEI Beta blockers Spironolactone if you live in Canada Control BP None of the above ICD’s MADIT study compared the ICD to conventional therapy in patients after myocardial infarction (MI) with an ejection fraction (EF) <35% and inducible VT beyond 3 weeks after MI. -54% reduction in overall mortality MUSTT which included a similar group of post-MI patients, revealed a 60% reduction in mortality compared to patients treated with antiarrhythmic medications. MADIT II included patients 4 weeks post-MI with LVEF ≤30%, and no EP study. ICD therapy resulted in a 31% reduction in overall mortality. These results confirmed that ICDs save lives in post-MI patients with reduced EF, without an EP study. The SCD-HeFT demonstrated that this benefit also extended to patients with NICM, NYHA class II/III HF and an EF <35% and NYHA class II/III HF symptoms. There was a 23% reduction of mortality with ICD therapy. CRT A systematic review of 14 randomized trials was published in 2007 by McAlister et al., evaluating 4,420 patients with LVEF <35%, QRS duration >120 msec, NYHA class III-IV HF, and optimal medical therapy. They reported that CRT improved LVEF by 3%, Improved LV remodeling, Quality of life, and exercise capacity, and 59% of patients had improvement by at least one NYHA class. Hospitalizations were decreased by 37%, And all-cause mortality was decreased by 22%. COMPANION CARE-HF 82 year old male-6 months later S/p ASMI 5 years ago with progressive DOE and edema History of hypertension and diabetes and smokes 1ppd Meds: Lasix 80/d, Lisinopril 40 mg, Coreg 25 mg BID, PE 92/60, p=79, RR=26 JVP 10 cm H20 +HJR Chest bilateral crackles and dull in right base Cor displaced PMI, 3/6MR murmur and S3; RV lift and TR murmur Abd-Liver 2FB below RCM and pulsatile Extr: 1+ edema EKG SR LBBB; QRS 161 ms Hb=10.1; Cr=2.2 , Bun 39, K=3.9, Echo: EF=22% , moderate to severe MR, moderate TR with TR velocity=3.6 m/s What else can be offered to this patient at this time? Single chamber ICD Dual chamber with backup pacing in RV Referral fp advanced therapy-ventricular assist device Cardiac resynchronization therapy (CRT) CRT-ICD What else can be offered to this patient at this time? Single chamber ICD Dual chamber with backup pacing in RV Referral fp advanced therapy-ventricular assist device Cardiac resynchronization therapy (CRT) CRT-ICD Serial Assessment Follow-up management of heart failure involves continued reassessment of symptoms, functional capacity, and therapeutic effectiveness, and continued evaluation for potentially exacerbating comorbidities. Routine evaluation of serum electrolytes and kidney function is recommended a minimum of every 6 months in clinically stable patients and more frequently with changes in therapy or clinical status. More frequent assessment of electrolytes and kidney function is indicated in patients with severe heart failure or who are clinically unstable and in patients on highdose diuretics or aldosterone antagonists. BNP Diagnostic if >100 Prognostic: Elevated levels are associated with worse prognosis across the spectrum of heart failure severity and provide further prognostic information in addition to peak exercise oxygen consumption and ejection fraction (EF) for predicting death Decompensated heart failure, a discharge BNP <300- reduced readmits. BNP>700 will have increased readmits. Assessing Prognosis Individual risk factors that correlate with poorer prognosis include Poor functional capacity as measured by NYHA functional class or peak oxygen uptake (VO2) on exercise testing, Hyponatremia, Hypotension Inability to tolerate ACE inhibitor or β-blocker treatment because of hypotension. Various composite risk scores have been developed to try to assess prognosis in ambulatory heart failure patients. Heart Failure Survival Score The Seattle Heart Failure Model is available online at www.SeattleHeartFailureModel.org, which allows health care providers and patients to quickly estimate 1-, 2-, and 5-year survival and to see what effect medical and device interventions have on estimated survival. Prognostic Indices HFSS The score is calculated from a number of variables , and patients are subsequently stratified into low, medium, and high risk. These strata correlate to one-year survival rates of 88%, 60%, and 35%, respectively. SHFM: Online score calculator that is readily accessible to most clinicians Acute Decompensated Heart Failure Sobering Facts HF hospitalization is associated with poor short- and long-term outcomes. In the ADHERE (Acute Decompensated Heart Failure National Registry) registry of over 107,000 HF hospitalizations, in-hospital mortality was 4%. In the EuroHeart Survey, 7% of the patients died during the hospitalization. Following a HF admission, mortality rates range from 8-14% at 30 days, to 26-37% at 1 year. Readmission with HF is also common, ranging from 20-25% at 60 days, to nearly 50% at 6 months. With each subsequent admission, the risk of dying increases OPTIMIZE CHF Precipitants for ADHF Acute chest pain and nonadherence to medications or diet were the precipitating factors in 33% and 21%, respectively. In the OPTIMIZE-HF registry, precipitating factors were identified in >60%, with pneumonia, ischemia, and arrhythmias being common. Inadequate therapy may be due to patient nonadherence, underutilization of ACEI/ARB’s and beta-blockers in HF, and diuretic doses may be decreased with worsening renal function. Comorbidities that may exacerbate HF symptoms and include uncontrolled hypertension and anemia. Acute kidney injury or worsening renal may further impair sodium or free water excretion and exacerbate fluid retention. Other potentially correctable factors include heavy alcohol consumption, and medications that cause myocardial depression or salt and water retention. ADHF Hemodynamic Profiles The most common hemodynamic profile in patients is congestion with normal perfusion. Symptoms respond to IV loop diuretic therapy. Vasodilator therapy may needed as elevated filling pressures can be exacerbated by systemic and pulmonary vasoconstriction. For patients who present with the combination of pulmonary and/or systemic venous congestion and systemic hypoperfusion, reduction in filling pressures and systemic vascular resistance can be accomplished with IV vasodilator therapy and diuretics. Conversion to an oral regimen that maintains stability of clinical and laboratory parameters may require 24-48 hours additional treatment. Hypoperfusion without congestion, manifested by progressive fatigue, and worsening renal function, may precipitate hospitalization with severe HF. Use of positive inotropic agents may be necessary. Cardiorenal Syndrome Coexistent cardiac and renal dysfunction is common in patients with HF. Reductions in renal blood flow and GFR lead to elevated levels of BUN and Cr. RAAS activation and diuretics may exacerbate renal dysfunction. During hospitalization, 15-30% will develop worsening renal function. Risk factors include age, diabetes, and renal impairment. Underlying mechanisms include diuretic-induced reductions in GFR, neurohormonal activation, and a fall in SBP. Worsening renal function may be transient or persistent, and often results in discontinuation of diuretics and RAAS inhibitors. In most studies, worsening renal function is an independent predictor of increased length of stay and excess inhospital and post-discharge mortality. Cardio-Renal Syndrome While congestion is often apparent, marked elevation in filling pressures may not be apparent due to increased pulmonary lymphatic drainage. DOE on minimal exertion or at rest, orthopnea and PND, are specific for increased left-sided filling pressures. In patients with biventricular HF, abdominal discomfort, nausea, and anorexia suggest increased right-sided filling pressures. Rales are a relatively specific, but insensitive, sign of pulmonary vascular congestion and are present in up to 2/3 of patients with ADHF, but also caused by coexistent pulmonary disease. Jugular venous distension is reliable indicator of increased left-sided filling pressures, ascites and peripheral edema are less sensitive Cardio-Renal Syndrome Like the physical examination, chest X-ray is an insensitive tool for detecting worsening HF. In the ADHERE registry, 19% had no signs of congestion on chest X-ray. When present, however, interstitial or alveolar edema suggests markedly elevated filling pressures. Pleural effusions are common in ADHF, and may not respond to diuresis. Fatigue and weakness, which are common complaints in HF, may be due to reduced cardiac output, poor perfusion of skeletal muscles, and respiratory muscle fatigue. Mental obtundation or anuria is highly suggestive of critically reduced perfusion. Other signs of systemic hypoperfusion include cool extremities, cyanosis, and a narrow pulse pressure with a thready pulse. Labs in Cardio-Renal Syndrome Increasing BUN/Cr K abnormalities high and low Hypomagnesemia Increased liver enzymes Hypoalbuminemia Elevated INR Low serum pre-albumin BNP’s: correlate modestly with LVFP’s. Changes may be predictive especially discharge BNP’s. Diuretics in ADHF Lasix 4 to 6x/day of doses 20-40 mg if lasix naiive If previous lasix use, dose exceeds chronic daily dose Hypomagnesemia and associated arrhythmias, metabolic alkalosis, muscle cramps, and exacerbation of gout. During IV diuresis, mild worsening of renal function may be tolerated in order to achieve hemodynamic compensation, and diuretic-induced hemoconcentration may be a marker for improved outcomes. Conversely, persistent worsening renal function may identify high-risk patients. Once treatment goals are achieved, the patient should be converted to an oral diuretic regimen. Tthe dose of IV diuretic that was effective may be given as an oral dose twice daily. Ultrafiltration For patients with marked fluid overload that is unresponsive to diuretics, or for those who develop worsening renal function requiring discontinuation of diuretics Ultrafiltration removes excess plasma volume without causing a significant change in electrolytes. In patients with chronic HF, reductions in peripheral and pulmonary edema, and a subsequent increase in diuretic efficacy have been reported. Recent studies have shown that frequent diuretic administration removes just as much fluid with less renal dysfunction 82 year old male S/p ASMI 5 years ago with progressive DOE and edema History of hypertension and diabetes and smokes 1ppd Meds: Lasix 40/d, Lisinopril 20 mg, Coreg 6.25 mg BID, Avandia, Meloxicam PE 92/60, p=108, RR=26 JVP 12 cm H20 +HJR Chest bilateral crackles and dull in right base Cor displaced PMI, MR murmur and S3 Abd-Liver 2FB below RCM and pulsatile Extr: 2+ edema EKG SR old anterior MI Hb=11.1; Cr=1.9 , Bun 31, K=3.9, total CO2=26 What is your 1st course of action when you see him in the hospital? Reduce Lisinopril as it is critically lowering the BP Decompensation due to inadequate beta blocker therapy-advance Coreg to 12.5 mg BID Begin decongesting patient low doses of furosemide to avoid hypotension (10 mg) Provide IV diuresis at a greater than oral dose but as IV (eg lasix 40 IV BID) Begin dobutamine to improve renal blood fow to augment diuresis What is your 1st course of action when you see him in the hospital? Reduce Lisinopril as it is critically lowering the BP Decompensation due to inadequate beta blocker therapy-advance Coreg to 12.5 mg BID Begin decongesting patient low doses of furosemide to avoid hypotension (10 mg) Provide IV diuresis at a greater than oral dose but as IV (eg lasix 40 IV BID) Begin dobutamine to improve renal blood fow to augment diuresis Cardiogenic Shock Cardiogenic shock is present when there is systemic hypotension and evidence for end-organ hypoperfusion, primarily due to inadequate cardiac output. Cardiogenic shock usually requires treatment with intravenous vasoactive medications and, in severe cases, device-based hemodynamic support. Manifestations of end-organ hypoperfusion may include acute kidney failure, elevated aminotransferases or hyperbilirubinemia, cool extremities, and decreased mental status. Therapeutic Options in Cardiogenic Shock Intravenous vasoactive medications are needed in the treatment of cardiogenic shock to augment cardiac output (inotropic agents) and to raise systemic blood pressure through peripheral vasoconstriction (vasopressors) If BP is acceptable, the addition of an intravenous vasodilator, to further increase cardiac output by reducing afterload. Use of these agents is generally limited to hours or days until shock resolves or more definitive therapy such as an intra-aortic balloon pump is instituted. Mechanical therapy for cardiogenic shock should be considered in patients with end-organ dysfunction that does not rapidly show signs of improvement (within the first 12-24 hours) Options for mechanical therapy include intra-aortic balloon pump and percutaneous or surgically implanted ventricular assist devices (VADs). Heart Failure Discharges and Readmits Up 259% since 1979 Readmits increased with comorbidities 50% patients do not lose weight in hospital (ADHERE) Progression of Underlying Disease Compliance Treatment Plan Inappropriate other medications At Discharge Addressed the exacerbating factors Achieved optimal volume staus Transitioned to oral diuretics Patient and Family Education 1 Week follow-up CMS Core Measures •Left ventricular function assessment •ACE inhibitor or ARB for left ventricular systolic dysfunction •Discharge instructions: symptom reporting, review of home medications, activity guidelines, diet guidelines, follow-up appointment, weight monitoring instructions •Adult smoking cessation advice/counseling Inpatient and Transitions of Care I IIa IIb III Throughout the hospitalization as appropriate, before hospital discharge, at the first postdischarge visit, and in subsequent follow-up visits, the following should be addressed: a. initiation of GDMT if not previously established and not contraindicated; b. precipitant causes of HF, barriers to optimal care transitions, and limitations in postdischarge support; c. assessment of volume status and supine/upright hypotension with adjustment of HF therapy, as appropriate; d. titration and optimization of chronic oral HF therapy; e. assessment of renal function and electrolytes, where appropriate; f. assessment and management of comorbid conditions; g. reinforcement of HF education, self-care, emergency plans, and need for adherence; and h. consideration for palliative care or hospice care in selected patients. Inpatient and Transitions of Care I IIa IIb III I IIa IIb III Multidisciplinary HF disease-management programs are recommended for patients at high risk for hospital readmission, to facilitate the implementation of GDMT, to address different barriers to behavioral change, and to reduce the risk of subsequent rehospitalization for HF. Scheduling an early follow-up visit (within 7 to 14 days) and early telephone follow-up (within 3 days) of hospital discharge is reasonable. I IIa IIb III Use of clinical risk prediction tools and/or biomarkers to identify patients at higher risk for postdischarge clinical events is reasonable. Mechanical Circulatory Support Some patients with severe refractory heart failure will need additional therapy because of progressive clinical deterioration. Mechanical devices have been developed to assist cardiac functioning primarily by taking over a portion of the cardiac output. Percutaneous VADs, placed in the cardiac catheterization laboratory and advanced to the left ventricle to provide partial circulatory support Surgically implanted VADs can be used longer (weeks to months or years).Indications for VAD placement include awaiting recovery from cardiogenic shock, as a bridge to cardiac transplantation, and as “destination therapy.” An inflow cannula in the left ventricular apex takes blood to the pump portion of the VAD, which returns blood to the aorta. Endorgan perfusion, quality of life, functional status, and survival are improved with VAD support for patients with end-stage heart failure. Complications of VADs include device malfunction, thromboembolism, infection, bleeding (with models requiring systemic anticoagulation), and hemolysis. Cardiac Transplant Cardiac transplantation is currently the best therapy available for end-stage heart failure in patients. One-year survival after cardiac transplantation is 85%, with median survival is 10 years. Diabetes, hypertension, dyslipidemia, and kidney disease are side effects from transplant medications. Many transplant medications (calcineurin inhibitors) also have significant drug interactions with common medications. Use of statins is associated with an increased risk for myositis. Azole antifungal agents and some CCB’s increase serum levels. As a consequence of chronic immunosuppression, patients are at increased risk for infections and cancer, frequently skin cancer and lymphoproliferative disease. Even high-grade rejection of the cardiac allograft may be asymptomatic or present with nonspecific findings such as atrial tachyarrhythmia. Overt LV dysfunction and clinical heart failure are generally late findings and require more intense inpatient immunosuppressive treatment. Cardiac Allograft Vasculopathy Cardiac allograft vasculopathy (CAV) is coronary disease of the cardiac allograft and is frequently limitsallograft longevity. CAV is characterized by diffuse intimal thickening of large epicardial and small terminal coronary branches, and is not amenable . Because of denervation cardiac transplant patients do not experience typical angina. Symptoms concerning for CAV in patients with a cardiac transplant include syncope, new heart failure symptoms, decreased exercise tolerance, dyspnea, and AVB New-onset heart failure symptoms should prompt concern for acute rejection or CAV. In select candidates, another cardiac transplantation is the only possible treatment, but outcomes are generally not as good as with first-time transplants