Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
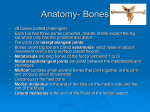
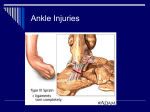
Chapter 15 Foot, Ankle, and Lower Leg Injuries Anatomy • 28 bones in the foot – Phalanges • Numbered 1-5 • Distal, middle, and proximal phalanges in each (except great toe) – Metatarsals • 1-5 • Metatarsophalangeal joint in between • Talus – Above the calcaneus • Calcaneus – Heel bone – Achilles attaches to posterior • Navicular • Cuboid • Medial, Intermediate, and • Lateral Cunieform Medial malleolus – Tibia (ankle) • Lateral Malleolus – Fibula (ankle) • Sesamoids – Floating bones – Tibial and fibular (usually 2) Arches of the foot • Longitudinal – From calcaneus to metatarsal heads – Functions: absorbing shock and balance • Metatarsal – Runs along metatarsal heads – Major weight bearing arch • Transverse – Located in front of the calcaneus, runs from 5th metatarsal to the navicular Longitudinal arches Muscles • There are 20 muscles in • the foot Tibialis anterior – Allows for dorsiflexion • Tibialis posterior – Helps with arch support • Peroneus longus and brevis – Foot eversion • extensors – Aid in dorsiflexion • flexors – Aid in foot plantarflexion and toe flexion Lateral Ankle Ligaments • anterior talofibular ligament – Prevents ankle from moving forward – Most commonly injured ligament in an inversion sprain • posterior talofibular • ligament calcaneofibular ligament – Aids in preventing ankle inversion Medial Ankle Ligaments • Deltoid ligament – Covers entire surface of the ankle – Maintains stability – Prevents extreme eversion – Stronger than all of the lateral ligaments combined Preventing foot, ankle, and lowerleg injuries • Protective measures – Supportive shoes worn correctly, taping, bracing – Maintenance of playing surface • Strengthening and conditioning programs – Proper stretching and strengthening prior to participation Treating foot, ankle, and lower-leg injuries and conditions • Ligament injuries – Great toe sprain (turf toe) – Arch sprain – Lateral and medial ankle sprains – Ankle dislocation • Great-toe sprain (turf toe) – injury to the joint capsule and ligaments of the metatarsophalangeal joint – Primary mechanism of injury (m.o.i) is hyperextension – Signs/symptoms: pain, tenderness and swelling, bruising and restriction of motion – Treatment: RICE, antiinflammatory, taping, stiff soled shoe; severe cases may be require surgery • Arch Sprain – MOI-prolonged activity on hard surfaces or with overuse – S/S-tenderness and swelling , and pain upon weight bearing – Treatment: RICE, antiinflammatory, supportive taping • Lateral ankle sprain – MOI-inversion, plantarflexion – S/S- swelling, discoloration, point tender over lateral ligaments – Treatment- RICE, antiinflammatory, refer for x-ray to r/o fx – Prevention- proper strengthening, taping, bracing • Medial Ankle sprains – MOI- eversion – S/S-swelling, discoloration, point tender over deltoid ligament – Treatment- RICE, antiinflammatory, refer for x-ray to r/o fx – Prevention- proper strengthening, taping, bracing • Ankle dislocation – MOIplantarflexion and forced inversion – S/S- deformity, swelling, pain – Treatment: immobilize, refer for xray/reduction – Immediate medical attention necessary Treating foot, ankle, and lower-leg injuries and conditions • Muscle and tendon injuries – Achilles tendinitis – Achilles tendon rupture Achilles tendinitis • Inflammation of the • • • achilles tendon MOI-overuse S/S- pain over achilles, swelling, may predispose athlete to tendon rupture Treatment-RICE, antiinflammatories, stretching, strengthening, taping Achilles tendon rupture • http://www.arthroscopy.c • • • om/achrup.avi MOI-sudden, unexpected force, or weakened achilles due to chronic tendinitis S/S-visual deformity, depression site, positive Thompson’s test Treatment- surgical repair or casting, often takes up to 6 months to heal Treating foot, ankle, and lower-leg injuries and conditions • Bone injuries • Fifth metatarsal avulsion fracture (Jones fracture) • Epiphyseal injury of distal tibia and fibula • Stress fracture Jone’s fracture (base of 5th metatarsal) • MOI-forced inversion and plantarflexion • S/S-pain, tenderness over base of 5th metatarsal, swelling • treament- nondisplaced fracture=conservati ve (boot), displaced=surgical repair Epiphyseal injury of distal tibia and fibula • Occurs in youth • MOI-supination and • • external rotation S/S-swelling, point tenderness, limited ROM Treatment-confirm w/xray, open or closed reduction, cast 4-6 weeks, full return to activity approx 3 months Stress fracture • MOI-repetitive stress (running, jumping) most often occur in tibia or metatarsal bones • S/S- point tenderness in specific area • Treatment-Rest, Ice, gradual return to activity, need bone scan or MRI to confirm • Prevention-increasing the level of exercise slowly, adequately warming up and stretching before exercise, and using cushioned insoles and appropriate footwear Treating foot, ankle, and lower-leg injuries and conditions • • • • • • • • • • Shin splints, or medial tibial stress syndrome Anterior compartment syndrome Contusions Toe abnormalities Bunions Plantar Fascitis Callouses Blisters Athlete’s foot Foot drop Shin splints and medial tibial stress syndrome • MOI-overuse, running on hard surfaces • S/S- point tenderness over the medial border of the leg • Treatment-conservative, RICE, condition often recurring, rehab • Prevention- supportive shoes, avoid running hills and hard surfaces Anterior compartment syndrome • Cause-muscle becomes • • • too big for the sheath that surrounds it causing pain MOI-direct impact that causes bleeding, muscle tear, overuse S/S- increased pain with exercise, pain with plantarflexion, weakness with dorsiflexion, swelling and tenderness over tibialis anterior Treatment-RICE, NSAIDs, orthodics, rehab, surgery Contusions • MOI-direct blow, • • • muscle tear S/S-pain, swelling, discoloration, limited function Treatment-RICE, compression Complication-myositis ossificans-damage to the muscle and bone periosteum causing new bone growth(calcification) within the muscle Toe abnormalities • Claw toe – Contracture of ligaments and tendons causing toes to curl downward • Hammer toe – Similar to claw toe, DIP joint less affected • Mallet toe – Inability to straighten DIP joint Cause: result from a muscle imbalance which causes the ligaments and tendons to become unnaturally tight Bunions • Causes-most common • • cause is wearing shoes that fit too tightly. They can also develop as a result of injury, stress on your foot or another medical condition. 10X more likely in women. Treatment-conservative steps that may include changing your shoes, padding your bunion and wearing shoe inserts, surgery an option as well. Prevention-wear shoes with a wide enough toebox Plantar Fasciitis • Causes-improper training, improper shoes, irregular arch, lack of flexibility in foot and lower leg • S/S-point tenderness either on the bottom or the back of the heel, possible limp, minimal swelling • Treatment-heel cup/lift, NSAIDs, ultrasound, stretching, modified activity Calluses • Causes-repeated • • • friction and pressure formed to protect the skin and the structures behind it from injury Treatment- soaking and sanding, moisturizer, shoe insoles or custom orthodics DO NOT cut or trim, seek MD advice/attn if diabetic Foot drop • Damage to the • • • peroneal nerve Inability to dorsiflex foot Treatment depends on actual cause Can be caused by other injury or surgery Athlete’s foot • skin disease caused by a • • • • • fungus, usually occurring between the toes warm, dark, and humid environment which encourages fungus growth S/S-are dry skin, itching, scaling, inflammation, and blisters can be spread to other parts of the body Treatment-Fungicidal and fungistatic chemicals Prevention- – Avoid walking barefoot; use shower shoes. – Reduce perspiration by using talcum powder. – Wear light and airy shoes. – Wear socks that keep your feet dry Blisters • Causes – Form as a result of heat, moisture and friction. – Friction forces caused by inappropriate footwear. – fungal infections of the skin, allergic reactions or burns. – Excessive foot perspiration. • Prevention-proper fitting • shoes/socks, keep feet dry, foot powder Treatment- drain if painful, apply antibiotic, do not remove protective “roof” skin, cover with bandaid