Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
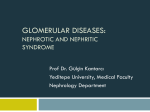
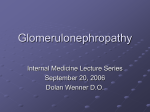
Nephrotic syndrome & GN Ebadur Rahman FRCP (Edin),FASN, Specialty Certificate in Nephrology(UK) MRCP(UK),DIM(UK),DNeph(UK),MmedSciNephrology(UK). Consultant & clinical tutor Department of Nephrology Riyadh Armed Forces Hospital Nephrotic syndrome This is characterized by proteinuria (Typically > 3.5g/24h), hypoalbuminemia ( less than 30g/dL ) and edema. Hyperlipidaemia. “nephrotic range” –nephrotic proteinuria Presentation New-onset oedema Initially periorbital or peripheral Later genitals, ascites, anasarca Frothy urine Generalised symptoms – lethargy, fatigue, reduced appetite Figure 1. Nephrotic edema. Heavy proteinuria (albuminuria) Further possible presentations... Oedema BP Leukonychia Breathlessness: Pleural effusion, fluid overload, AKI,PE,MI. DVT Eruptive xanthomata/ xanthalosmata Hemoconcentration Immobility, especially in patients with anasarca thrombocytosis, increased platelet activation, decreased levels of antithrombin, free protein S, and plasminogen (due to urinary losses), NEPHROTIC SYNDROME Secondary - Primary glomerular disease Primary glomerular disease PRIMARY NEPHROTIC SYNDROME Minimal Change Disease- commonest in children Focal Segmental Glomerulosclerosis Membranous Nephropathy- commonest in adult Membranoproliferative Glomerulonephritis(MPGN) Iga nephropathy RARE to cause nephrotic syndrome but commonest GN For exam Minimal change gn Membranous gn Amiloidosis SLE DM Urine dipstick The urine sediment (or direct counting of RBC per mL of uncentrifuged urine) is the gold standard for the detection of microscopic hematuria. Dipsticks for heme detect 1 to 2 RBCs per high power field false positive tests due to the following: Semen is present in the urine after ejaculation and may cause a positive heme reaction on the dipstick [ urine pH greater than 9 or contamination with oxidizing agents used to clean the perineum The presence of myoglobinuria False negative tests have been reported in patients ingesting large amounts of vitamin C Isolated glomerular hematuria Renal biopsy is not usually performed there is no specific therapy for these conditions renal prognosis is excellent management of these patients is not usually affected by the biopsy When renal biopsy is performed in such patients, the most common findings-are a normal biopsy IgA nephropathy, Thin basement membrane disease (benign familial hematuria), mild nonspecific glomerular abnormalities, Alport syndrome All patients should have a urine culture to exclude infection prior to evaluation of hematuria. Hyperlipidemia total cholesterol and low-density lipoprotein (LDL) Lipoprotein (a) [Lp(a)] high-density lipoprotein (HDL) cholesterol . Renal biopsy Nephrotic syndrome Nephritic syndrome Unexplained renal impairement Vasculitis where kidneys are commonly involved Renal allograft dysfunction Percutaneous renal biopsy is generally contraindicated in the following settings: Uncorrectable bleeding diathesis Small kidneys which are generally indicative of chronic irreversible disease Severe hypertension, which cannot be controlled with antihypertensive medications Multiple, bilateral cysts or a renal tumor Hydronephrosis Active renal or perirenal infection An uncooperative patient Table 4 In children- diagnosis of MCD is usually made based upon the clinical. Almost all children with MCD respond to a short course of glucocorticoids. it is considered steroid-resistant (SR-NS) when no remission is achieved after about two months of full-dose steroid therapy. Pediatricians usually restrict renal biopsy to individuals with SR-NS The clinical findings at presentation in adults Proteinuria – nephrotic range Hematuria – 29 percent Hypertension – 43 percent Acute renal failure – 18 percent PRIMARY NEPHROTIC SYNDROME Minimal Change Disease Focal Segmental Glomerulosclerosis Membranous Nephropathy Membranoproliferative Glomerulonephritis(MPGN) Figure 6. Light microscopic appearances in focal segmental glomerulosclerosis. Segmental scars with capsular adhesions in otherwise normal glomeruli. Table 5 PRIMARY NEPHROTIC SYNDROME Minimal Change Disease Focal Segmental Glomerulosclerosis Membranous Nephropathy Iga nephropathy Membranoproliferative Glomerulonephritis(MPGN) Membranous nephropathy (MN) - one-third of biopsy diagnoses in adult nondiabetics diffuse thickening of the glomerular basement membrane (GBM) on light microscopy, "spikes" on silver stain, diffuse granular IgG and complement deposition on immunofluorescence, and subepithelial dense deposits on electron microscopy Antibodies to the M-type phospholipase A2 receptor (PLA2R ) are found in a high proportion of patients with primary (idiopathic) MN. Most patients with MN present with the nephrotic syndrome with normal or near normal serum creatinine. 10% associated with malignancy Table 6 Figure 7a. Early MN: a glomerulus from a patient with severe nephrotic syndrome and early MN, exhibiting normal architecture and peripheral capillary basement membranes of normal thickness (Silver–methenamine ×400). Figure 7b morphologically advanced MN Figure 7c. Morphologically more advanced MN (same patient as in (b)) IgA nephropathy most common cause of primary glomerulonephritis. in Asians and Caucasians. There is a 2:1 male to female predominance IgA nephropathy is characterized by prominent, globular deposits of IgA in the mesangium on immunofluorescence microscopy. Electron microscopy shows dense deposits primarily in the mesangium Most patients with IgA nephropathy present with either visible hematuria (single or recurrent), usually following an upper respiratory infection, or invisible hematuria with or without mild proteinuria incidentally detected on a routine examination 40 to 50 percent present with one or recurrent episodes of visible hematuria, usually following an upper respiratory infection Another 30 to 40 percent have microscopic hematuria and usually mild proteinuria, and are incidentally detected on a routine examination Less than 10 percent present with either nephrotic syndrome or rapidly progressive glomerulonephritis A kidney biopsy only protein excretion above 0.5 to 1 g/day, elevated serum creatinine concentration, or hypertension. PRIMARY NEPHROTIC SYNDROME Membranoproliferative Glomerulonephritis(MPGN) Figure 8. Pathology of membranoproliferative glomerulonephritis type I. (a) Light microscopy shows a hypercellular glomerulus with accentuated lobular architecture and a small cellular crescent (methenamine silver). Table 7 Diagnosis fasting blood sugar and glycosylated hemoglobin antinuclear antibody test serum complement, In selected patients, cryoglobulins, hepatitis B and C serology, anti-neutrophil cytoplasmic antibodies (ANCAS), anti GBM antibodies, renal biopsy to define the pattern of glomerular involvement. Complications Infection Coagulation disorders Protein malnutrition and dyslipidemia Acute renal failure Treatment General treatment 1. 1. Relief edema 2. Rx Htn 2. Symptomatic treatment Treating dyslipidemias, anticoagulate treatment, 3. Immunosupressive treatment