Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
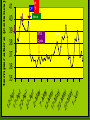
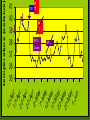
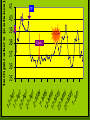
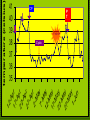
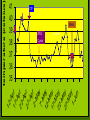
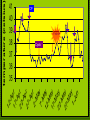
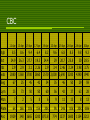
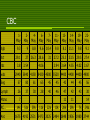
MEDICAL GRANDROUNDS July 3, 2008 Abigail Cruz-Zaraspe M.D. OBJECTIVES To present a case of bacteremia in aplastic anemia To discuss salmonella nontyphi bacteremia and myositis manifestations, diagnosis and treatment To discuss briefly the treatment of aplastic anemia IDENTIFYING DATA A.R. 42/M Married Real-estate broker CHIEF COMPLAINT Right thigh pain HISTORY OF PRESENT ILLNESS 5 weeks PTA 4 weeks PTA Easy fatigability, SOB, (+) melena, (+) abdominal pain, (+)palpitations sought consult, CBC Pancytopenia admitted for the first time for transfusion HISTORY OF PRESENT ILLNESS First admission blood transfusions BMA-hypocellular BM Dx: Aplastic anemia treatment options were discussed (discharged-platelet ct 44k) HISTORY OF PRESENT ILLNESS 3 weeks PTA intermittent fever (390C),body malaise, nose bleeding Consult: WBC 1860, PLT 10k Tx: Co-amoxyclav 625mg TID x7d, tranexamic acid 500mg TID GCSF 300mcg HISTORY OF PRESENT ILLNESS 3 weeks PTA 2nd admission generalized petechial rashes & gum bleeding and was admitted CBC- pancytopenia Tx: blood & PC transfusions CBC on SECOND ADMISSION hgb hct wbc stabs segmenter lymphocyte platelet ct anc 22-Mar 8.5 25.5 1850 24-Feb 8 24.4 2960 25-Mar 10 30.5 2190 54 40 5000 999 72 23 2000 2131 48 45 14000 1051 HISTORY OF PRESENT ILLNESS 2nd admission Initially given Cefepime 1gm Q12 HISTORY OF PRESENT ILLNESS 2nd admission + right thigh & hip pain 5/10 (dull, aching constant) +direct tenderness no swelling no limitation in ROM no paresthesia Hip & Thigh pain Compartment syndrome Avascular necrosis neuropathy infection fracture NEUROPATHY Severe intractable pain Unusual burning, tingling or shocklike quality Triggered by light touch Sensory deficit on area of pain Hip & Thigh pain Compartment syndrome Avascular necrosis neuropathy infection fracture COMPARTMENT SYNDROME Pain Parasthesia Pulselessness Pallor pressure Hip & Thigh pain Compartment syndrome Avascular necrosis neuropathy infection fracture HISTORY OF PRESENT ILLNESS 2nd admission Pelvis and Right hip xray: no pathologic finding Hip & Thigh pain Compartment syndrome Avascular necrosis neuropathy infection fracture HISTORY OF PRESENT ILLNESS 2nd admission Blood CS: Salmonella enteritidis Grp C Sensitive: Ceftriaxone Chloramphenicol Ciprofloxacin shifted to Ciprofloxacin 500mg/tab, 1 tab BID HISTORY OF PRESENT ILLNESS 2nd admission Dx: Aplastic anemia Salmonella nontyphi bacteremia Advised treatment w/ Anti-thymocyte globulin / cyclosporine HISTORY OF PRESENT ILLNESS 2nd admission THM: Ciprofloxacin 500mg/tab, 1 tab BID to complete 7 days Prednisone 30mg BID, Tranexamic acid & Omeprazole HISTORY OF PRESENT ILLNESS Since discharge episodes of fever & progression R hip & thigh pain on movement & palpation unable to stand admitted 3rd time REVIEW OF SYSTEMS (-) headache (-) loss of consciousness (-) cough or colds (-) weight loss (-) chest pain (-) dyspnea (-) palpitations (-) abdominal pain (-) nausea or vomiting (-) LBM/ constipation (+) melena (-) hematochezia (-) dysuria (-) hematuria PAST MEDICAL HISTORY Non-hypertensive Non-diabetic No known allergies FAMILY HISTORY No No No No No hypertension diabetes asthma blood dyscrasias cancer PERSONAL AND SOCIAL HISTORY Previous smoker, stopped in late ‘90s Occasional beer drinker Lived near an electroplating factory Previously worked as a cashier in a gasoline station Real estate broker PHYSICAL EXAMINATION General: conscious, coherent, bed-bound Vital signs: BP 130/80, HR = 103 bpm, reg, RR = 22/min, T = 390C HEENT: Pale conjunctivae, icteric sclerae, no tonsillopharyngeal congestion, no cervical lymphadenopathy PHYSICAL EXAMINATION Chest/Lungs: Symmetrical chest expansion, no retractions, clear breath sounds Adynamic precordium, tachycardic with regular rhythm, no murmurs PHYSICAL EXAMINATION Abdomen: Flabby, normoactive bowel sounds, soft, non-tender, no hepatomegaly no splenomegaly PHYSICAL EXAMINATION Extremities: (+) erythema and hyperemia, right thigh extending to mid-leg area No discharge, no open wounds no sensory deficit Left leg was grossly normal pulses: full and equal SALIENT FEATURES 42/M Known case of aplastic anemia Known case of non-typhi salmonella bacteremia Treated with ciprofloxacin 500mg BID x 1 week Still febrile Right thigh and hip pain Erythema and swelling of right lower extremity Hip & Thigh pain Compartment syndrome Avascular necrosis neuropathy infection fracture AVASCULAR NECROSIS results from infarction of bone trabeculae and marrow cells equal frequency in the femoral and humeral heads The femoral heads more commonly undergo progressive joint destruction as a result of chronic weight bearing. The changes are best detected by MRI AVASCULAR NECROSIS Most studies have found that the risk is low (< 3 percent) in patients treated with doses of prednisone less than 15 to 20 mg/day In one series, the prednisone dose in the highest month of therapy exceeded 40 mg/day in 93 percent, and 20 mg/day in 100 percent of patients with osteonecrosis. Hip & Thigh pain Compartment syndrome Avascular necrosis neuropathy infection fracture 150 patients with aplastic anemia treated at Clinical Hematology Branch of the National Heart, Lung and Blood Institute (NHLBI) between 1978 and 1990 Infection was documented in 47% of cases respiratory tract (32 percent) soft tissues (24 percent) blood (22 percent) gastrointestinal tract (17 percent) urinary tract (6 percent). IMPRESSION Aplastic anemia Salmonella non-typhi bacteremia with secondary myositis r/o Avascular necrosis, osteomyelitis COURSE IN THE WARDS On admission CBC, PT, PTT, UA, CXR, crea, BUN, K, Na were requested. He was placed on a neutropenic diet. He was started on Piperacillintazobactam 4.5mg/IV x 1dose then 2.25mg q8 hours LABS APRIL 12, 2008 hgb hct rbc wbc metamyelocytes stabs segmenter lymphocyte mono platelet ct anc 12-Apr 8.5 24.9 2.9 2880 1 67 25 7 6000 1929 12-Apr na k bun crea CXR- normal 134 4.2 21 1.2 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 Piperacillin-tazobactam 40 39 38 37 36 35 Febrile COURSE IN THE WARDS 2nd hospital day + severe leg pain, unrelieved by Tramadol. referred to Orthopedic service Impression: t/c pathologic fracture vs. avascular necrosis, R hip; aplastic anemia. Tx: Ketorolac and Morphine. COURSE IN THE WARDS 2nd hospital day Pelvic MRI was requested Myositis with fasciitis involving the right gluteal and right thigh muscle and the right obturator internus muscle. Avascular necrosis of the right femoral head considered COURSE IN THE WARDS 2nd hospital day still with fever and leg pain Blood CS: Salmonella Enteritidis Group C sensitive to Ceftriaxone and Ciprofloxacin resistant to Co-trimoxazole and Ampicillin. COURSE IN THE WARDS 5th HD referred to Infectious Disease service. Impression: Salmonella nontyphi bacteremia with secondary myositis. Tx: shift Piperacillin-tazobactam to Ciprofloxacin 500mg/tab 2x a day & ceftriaxone 2g/IV OD 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 P 40 T 39 38 37 36 35 CP & CT Febrile COURSE IN THE WARDS 11th HD patient was still febrile (Tmax400C) endovascular Salmonella was considered Ceftriaxone was discontinued Piperacilin-Tazobactam was resumed & increased to 4.5 IV Q8 dexamethasone 4mg/tab 12 hrs 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 P 40 T 39 38 37 36 35 CP+CT CP CT dexa Febrile COURSE IN THE WARDS 13th HD Afebrile pain decreased Dexamethasone was tapered to 4mg/tab bid. COURSE IN THE WARDS 18th HD Cyclosporine (Neoral)100mg/cap BID ATG 1000mg in PNSS x 4 hrs, once daily until D11 ( 5/9/08) 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 40 39 38 37 36 35 P CP T dexa ATG Febrile Cyclo COURSE IN THE WARDS 21st HD patient was afebrile, Piperacillin-tazobactam was discontinued 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 40 39 38 37 36 35 P CP T P T Febrile ATG ATG Cyclo COURSE IN THE WARDS 38th HD fever recurred Increased severity of R thigh pain Blood CS: negative after 5 days CBC still showed pancytopenia. 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 40 39 38 37 36 35 CP Febrile Cyclo COURSE IN THE WARDS 41st HD persistence of fever CXR,urinalysis,CBC were requested CXR & urinalysis were normal CBC still showed pancytopenia. Piperacillin-tazobactam 4.5g/IV q8 was resumed 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 40 39 38 37 36 35 CP P T Febrile Cyclo COURSE IN THE WARDS 46th HD BMA: beginning bone marrow recovery. Some section shows good cellularity with myeloid and erythroid precursors, although megakaryocytes are still decreased but present 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 40 39 38 37 36 35 CP BMA ATG Febrile Cyclo BMA ATG DATE platelet ct /0 8 5/ 27 /0 8 5/ 22 /0 8 5/ 17 /0 8 5/ 12 08 5/ 7/ 08 5/ 2/ /0 8 4/ 27 /0 8 4/ 22 /0 8 Cyclo 4/ 17 /0 8 80000 75000 70000 65000 60000 55000 50000 45000 40000 35000 30000 25000 20000 15000 10000 5000 0 4/ 12 PLATELET COUNT PLATELET COUNT date 6/1/08 5/27/08 5/22/08 5/17/08 5/12/08 5/7/08 5/2/08 6000 5500 5000 4500 4000 3500 3000 2500 2000 1500 1000 500 0 4/27/08 4/22/08 4/17/08 4/12/08 anc anc ATG Cyclo anc COURSE IN THE WARDS 47th HD again had febrile episodes Blood culture: negative MRI of R leg: myositis, fasciitis & avascular necrosis of the R thigh 12 -A p 17 r -A 22 pr -A pr 27 -A pr 2-M ay 7-M 12 ay -M a 17 y -M 22 ay -M a 27 y -M ay 1-J un temperature (celsius) 41 40 39 38 37 36 35 CP Febrile Cyclo COURSE IN THE WARDS 53rd HD sent home afebrile medications: Tranexamic acid, Cyclosporine 100mg BID, ciprofloxacin 500mg BID FINAL DIAGNOSIS Aplastic anemia Salmonella enteritides myositis Avascular necrosis, femoral head DISCUSSION SALMONELLA: MICROBIOLOGY Gram-negative non-spore forming Facultatively anaerobic bacilli Produce acid on glucose fermentation Motile Do not ferment lactose (99%) Differential metabolism of sugars is used to distinguish serotypes S. typhi does not produce gas on sugar fermentation NON-TYPHOIDAL SALMONELLA: EPIDEMIOLOGY 1996-1999 estimated 1.4M cases of NTS in US 2004 – 14.7/100,000 persons Typhimurium – 20% Enteritidis – 15% Newport – 10% NON-TYPHOIDAL SALMONELLA: EPIDEMIOLOGY - HOST FACTORS Impaired cell-mediated immunity AIDS Corticosteroid use Malignancy Impaired phagocytic function Hemoglobinopathies Chronic granulomatous disease Schistosomiasis Histoplasmosis Malaria NON-TYPHOIDAL SALMONELLA: EPIDEMIOLOGY - HOST FACTORS Neonates Elderly Extremes of ages Decreased gastric acidity achlorhydria Antacids or suppression of gastric acidity Altered intestinal function IBD Prior antibiotic therapy NON-TYPHOIDAL SALMONELLA: EPIDEMIOLOGY Small but significant number Associated with food products (meat, poultry, eggs or dairy products) Associated with shell eggs Associated with exotic pets, especially reptiles NON-TYPHOIDAL SALMONELLA: EPIDEMIOLOGY NON-TYPHOIDAL SALMONELLA: PATHOGENESIS Ingestion from contaminated food/water Infectious dose: 103-106 CFU Gastric acidity is the initial barrier Bacteria mediated endocytosis NON-TYPHOIDAL SALMONELLA: PATHOGENESIS Innate immune system May be determining factor for severity Depressed PMN function increases incidence Cell-mediated immunity Role in clearing infection and protecting against subsequent Salmonella infection Humoral immune responses Protective immunity NON-TYPHI SALMONELLA CLINICAL MANIFESTATIONS • • • • Gastroenteritis Bacteremia and vascular infection Localized infection Chronic carrier state Clinically useful, have no pathogenic nor prognostic significance NON-TYPHI SALMONELLA BACTEREMIA AND VASCULAR INFECTIONS 5% of patients with NTS Infants, elderly and immunocompromised Salmonella has high propensity for infection of vascular sites 10-25% in persons > 50 Aorta Venous septic thrombophlebitis NON-TYPHI SALMONELLA : LOCALIZED INFECTION Occurs in 5-10% of patients with NTS bacteremia NON-TYPHI SALMONELLA : LOCALIZED INFECTION NON-TYPHI SALMONELLA : LOCALIZED INFECTION NON-TYPHI SALMONELLA SPECIAL POPULATIONS Immunosuppression Biliary and urinary tract abnormalities Hemoglobinopathies Malaria Schistosomiasis Histoplasmosis AIDS NON-TYPHI SALMONELLOSIS TREATMENT Neonates, >50 years of age and in patients with immunosuppresion or valvular/endovascular abnormalities Oral or IV antimicrobial for 48 to 72 hours or until patient is afebrile SALMONELLA NON-TYPHI BACTEREMIA TREATMENT Empiric: 3rd generation cephalosporin and a fluoroquinolone Low-grade: 7-14 days of Tx High-grade: 6 weeks IV therapy with ßlactam (ampicillin or ceftriaxone) is recommended to treat documented or suspected endovascular infection IV Ciprofloxacin, followed by prolonged oral therapy SALMONELLA NON-TYPHI LOCALIZED INFECTION TREATMENT Ceftriaxone 2g/d or Cefotaxime 2g q8h Ciprofloxacin 500mg/tab BID or 400mg/IV BID Ampicillin 2g/IV q6h SALMONELLA: ANTIMICROBIAL RESISTANCE Widespread use of “over-the-counter” antibiotics Plasmid-encoded resistance Empirical treatment of febrile syndromes and as growth promoters in animal production DT104: resistant to ACSSuT: ampicillin, chloramphenicol, streptomycin, sulfonamides and tetracyclines Acquired from plasmids in Pseudomonas species SALMONELLA: ANTIMICROBIAL RESISTANCE Increase in ceftriaxone and fluoroquinolone resistant nontyphoidal Salmonella SALMONELLA: PREVENTION AND CONTROL Hand washing Safe drinking water and effective sewage treatment Improved food safety practices Good personal hygiene Prudent antimicrobial use TREATMENT OF APLASTIC ANEMIA Hematopoietic stem cell transplantation Immunosuppression Anti-thymocyte globulin – induces hematologic recovery Addition of cyclosporine increases response rate up to 70% esp. in children Improvement in leukocyte count apparent within 2 months TREATMENT OF APLASTIC ANEMIA (IMMUNOSUPPRESSIVE THERAPY) improvement in blood counts occurred in 60 percent of patients after three months The actuarial risk of relapse was 35 percent at five years. Most of the relapsing patients responded to additional courses of immunosuppression, and relapse was not associated with a significant survival disadvantage.. Rosenfeld, SJ, Kimball, et.al Intensive immunosuppression with antithymocyte globulin and cyclosporine as treatment forsevere acquired aplastic anemia. Blood 1995; 85:3058. Treatment of aplastic anemia with antilymphocyte globulin and methylprednisolone with or without cyclosporine. The German Aplastic Anemia Study Group antilymphocyte globulin, methylprednisolone, and cyclosporine appears to be more effective than a regimen of antilymphocyte globulin and methylprednisolone without cyclosporine may thus represent a treatment of choice for patients who are not eligible for bone marrow transplantation Frickhofen N, Kaltwasser JP, Schrezenmeier H, Raghavachar A, Vogt HG, Herrmann F, Freund M, Meusers P, Salama A, Heimpel H THANK YOU! CBC 12-Apr 13-Apr 15-Apr 17-Apr 19-Apr 23-Apr 25-Apr 26-Apr 28-Apr 30Apr hgb 8.5 8.6 9.4 6.4 8.2 9.6 6.8 8.5 9.8 9.3 hct 24.9 26.3 27.7 19.3 24.4 29 20.7 25.8 30 28.5 rbc 2.9 2.9 3.1 2.26 2.9 3.4 2.46 3.24 3.98 3.75 wbc 2880 1360 3700 2860 2570 2,000 2,690 3200 4290 1940 Seg 67 25 45 42 34 35 46 50 29 59 Lym 25 73 50 50 60 56 42 37 63 28 Mon 7 2 5 8 6 9 11 13 8 13 Plate 6k 16k 10k 15k 20k 9k 24k 10k 20k 10k 1929 340 1665 1200 873.8 774 1237 1600 Anc 1154 2212 CBC 1May 2May 4May 6May 7May 11May 13May 14May 19May 22May hgb 9.3 9 8.8 9.6 10.4 9.8 8.1 11.1 9.8 9.1 hct 29.1 27 26.3 28.6 31 27.2 25.3 33.5 29.5 27.4 rbc 3.8 3.54 3.94 3.64 4.55 4.02 3.67 wbc 4.06 2940 5840 4150 8420 4500 5520 4400 4400 4400 4900 Seg 57 80 61 65 45 45 42 44 45 56 Lymph 26 37 30 28 40 46 47 42 43 30 Mono 7 11 11 . PC Anc 14k 51k 39k 11k 22k 10k 28k 29k 14 7k 74k 1675 4192 2531 5473 2025 2484 1848 1936 1980 2744 TREATMENT OF APLASTIC ANEMIA (IMMUNOSUPPRESSIVE THERAPY) Horse ATG at a dose 40 mg/kg per day in 500 mL of saline given over four to six hours for four consecutive days. Rosenfeld, SJ, Kimball, et.al Intensive immunosuppression with antithymocyte globulin and cyclosporine as treatment forsevere acquired aplastic anemia. Blood 1995; 85:3058. TREATMENT OF APLASTIC ANEMIA (IMMUNOSUPPRESSIVE THERAPY) Prednisone or methylprednisolone in divided doses of 1 mg/kg per day. Steroids were given for two weeks, with the dose tapered so that the corticosteroids were discontinued by day 30. Rosenfeld, SJ, Kimball, et.al Intensive immunosuppression with antithymocyte globulin and cyclosporine as treatment forsevere acquired aplastic anemia. Blood 1995; 85:3058. TREATMENT OF APLASTIC ANEMIA (IMMUNOSUPPRESSIVE THERAPY) Cyclosporine, 10-12 mkd, in two equally divided doses, aiming for trough levels of 100 to 200 ng/mL of serum or 500 to 800 ng/mL in whole blood. Cyclosporine is generally continued for about six months, although the dose may be tapered after one month to trough whole blood levels of 200 to 500 ng/mL. Rosenfeld, SJ, Kimball, et.al Intensive immunosuppression with antithymocyte globulin and cyclosporine as treatment forsevere acquired aplastic anemia. Blood 1995; 85:3058.





































































































![Aplastic Anemia [PPT]](http://s1.studyres.com/store/data/000248384_1-5c39883593ffaaa864ec61d1eb51b312-150x150.png)