Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
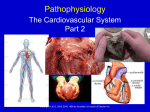
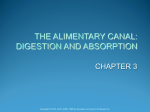
Assisting in Urology and Male Reproduction Chapter 39 Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. The Urinary System Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 2 Urinary System Urinary system—two kidneys located bilaterally in the retroperitoneum, two ureters, urinary bladder, and urethra. Functions include: – Maintain water-electrolyte balance – Activate vitamin D – Secrete erythropoietin for RBC production – Regulate blood pressure through renin Primary function is to remove waste products from blood and form urine for secretion. – Byproducts of metabolic processes – Salts and nitrogenous wastes Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 3 Kidney Anatomy and Physiology Cortex—outer layer of kidney contains the nephron unit. Urine passes from the cortex to the calyxes, which are the distal collection areas of the renal pelvis. Emptied through bilateral ureters to urinary bladder. When the bladder is full, sphincters open, and urine flows into the urethra. Urethra 20 cm long in males and 3 to 4 cm in female; urine passes through the urinary meatus. Micturition. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 4 Urine Production Three processes are involved in urine formation: filtration, reabsorption, and excretion. Filtration and reabsorption occur in the nephron unit – Glomerulus – Partially surrounded by Bowman’s capsule – Fluid and dissolved substances pass into Bowman’s capsule – Continues into convoluted tubules where reabsorption occurs – Then on to the collecting tubules in the medulla – Urine excreted starting from the calyx outward Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 5 The Kidney Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 6 Disorders of the Urinary System The urinary tract has a continuous mucosal lining, which gives organisms that enter the urethra a direct pathway through the system. Most common symptoms of renal system disorders: – Changes in the frequency of urination – Dysuria – Urgency – Retention – Incontinence Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 7 Diagnosis of Urinary System Disorders Urinalysis, blood urea nitrogen (BUN) levels, and analysis of creatinine clearance Kidney-ureter-bladder radiograph (KUB)—flat plate of abdomen; shows size, shape, location, and malformations of kidneys and bladder Renal scanning—nuclear scans to determine size, shape, and function of kidney; used to diagnose renal obstruction or hypertension Cystography—radiograph with contrast dye to study the bladder Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 8 Diagnostic Procedures • Intravenous pyelogram (IVP)—x-ray taken at intervals after dye is injected intravenously to visualize the urinary system; used to diagnose tumors, calculi, or obstructions • Renal arteriogram—dye injected into renal artery to show kidney blood flow • Renal computed tomography—provides transverse views of the kidneys to detect tumors, abscesses, or hydronephrosis Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 9 Diagnostic Procedures (cont’d) • Renal ultrasound—high frequency sound waves used to detect functional defects in the kidneys or polycystic disease. • Cystoscopy—endoscopic view of the urethra and bladder for biopsy, to find or remove calculi, or to place renal stents. • Retrograde pyelogram—visualizes renal system after injection of dye into bladder, ureters, or kidneys. • The Medical Assistant needs to understand the patient preparation for each diagnostic procedure. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 10 Urinary Incontinence A temporary or chronic loss of urinary control Causes vary – Infections, brain disorders, tissue damage – Stress incontinence Treatment methods for incontinence depend on the causative factor – Kegel exercises, antispasmodic medications, catheters – Surgical intervention Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 11 Urinary Infections and Inflammation Most urinary tract infections (UTIs) are ascending; start with pathogens in perineal area infecting the continuous mucosa up through urethra, bladder, ureters, to kidneys. Infection and inflammation of urethra is urethritis; that of bladder is cystitis; resident bacteria of the colon, Escherichia coli, is the usual causative agent. Women anatomically at greater risk because of close relation of anus and urethra. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 12 General UTI Signs and Symptoms An overwhelming urge to urinate Burning on urination Urgency with frequent, small amounts of urine Blood in the urine (hematuria) or cloudy, dark, foulsmelling urine Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 13 UTIs Continued Pyelonephritis—inflammation of renal pelvis and kidney; caused by ascending bacterial infection Conditions such as urinary retention or obstruction promote urinary stasis and growth of bacteria UTI treatment: – Antibiotics—Keflex, Bactrim – Force fluids – Proper hygiene – Empty bladder completely – Cranberry juice Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 14 Glomerulonephritis Acute—degenerative inflammation of glomeruli; develops in children and adolescents about 2 weeks after strep infection – Low-grade fever, anorexia, flank pain, hypertension, edema – Hematuria and proteinuria – Treatment: diuretics Chronic—causes progressive, irreversible renal damage; may result in renal failure; caused by antigen-antibody reaction that destroys the nephron unit – Hypertension, hematuria, proteinuria, oliguria, edema – Only cure is kidney transplant Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 15 Renal Calculi Renal calculi—created when salts in urine collect in the kidney or when fluid intake is low, creating a highly concentrated filtrate; are common and tend to recur if the cause of formation is not treated Small stones usually do not cause any difficulty until they grow large enough to lodge in the ureters or renal pelvis. Very painful if passed. Blockage can result in: – Hydronephrosis – Dilation of calyxes and increased pressure on nephron units Treatment: cystoscopy, extracorporeal shockwave lithotripsy (ESWL) Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 16 Shock-wave Lithotripsy Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 17 Hydronephrosis The swelling of the kidney caused by the inability of urine to drain out of the renal pelvis; is usually caused by blockage from renal calculi but may also result from an enlarged prostate or a tumor Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 18 Hydronephrosis (cont’d) Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 19 Polycystic Disease Autosomal dominant genetic disorder. Slowly progressive and irreversible. Causes formation of multiple grapelike cysts in the kidneys. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 20 Polycystic Disease (cont’d) Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 21 Polycystic Disease As cysts enlarge, they compress surrounding tissue, causing necrosis, uremia, and renal failure. Patients have family history of disease. Symptoms develop as patient ages—adolescence or early adulthood. Will eventually require renal dialysis or transplant. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 22 Bladder Cancer Most common cancer of urinary tract. Two to three times more common in men. Risk increases with smoking, recurrent UTIs, exposure to carcinogens, large amounts of analgesics. Characterized by one or more tumors that can recur. Tumors are invasive and can metastasize through the blood or surrounding pelvic lymph nodes. NMP22 urine test diagnostic for recurrence. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 23 Neoplasms of the Urinary Tract Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 24 Renal Carcinoma Adenocarcinoma of the kidney – Primary tumor initially asymptomatic – Frequently has metastasized before being diagnosed – Typically seen in men over 50 and smokers Wilms’ tumor – Cancer of kidney in children – Results from an inherited genetic defect – Occurs unilaterally at about 2 to 5 years of age – 90% survival rate Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 25 Renal Failure Acute—sudden, severe onset; caused by exposure to toxic chemicals, severe or prolonged circulatory or cardiogenic shock from serious burns or heart disease, or from an acute bilateral kidney infection or inflammation. Primary problem must be resolved as quickly as possible to prevent permanent renal failure. Chronic—slowly progressive process; caused by the gradual destruction of nephron unit. Three stages ending in end-stage renal failure requiring dialysis or transplant. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 26 Dialysis Dialysis, or cleansing of the blood, is used to treat acute renal failure until the problem is reversed or, for those patients in end-stage renal disease, until a transplant can be done. Hemodialysis. Peritoneal dialysis. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 27 Dialysis (cont’d) Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 28 Pediatric Urologic Disorders Enuresis—inability to control urination or bedwetting; may be caused by physical or psychologic disorders Cryptorchidism—failure of one or both testes to descend into the scrotum; can result in male infertility; may be corrected with an orchiopexy Urine reflux disorder—backward flow of urine into the ureters when voiding; usually caused by an infection. Treatment includes: – Prophylactic antibiotics – Surgical repair of ureters Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 29 Anatomy and Physiology of the Male Reproductive System Made up of a pair of testes located in the scrotum. Testes contain seminiferous tubules, where spermatozoa are produced. Sperm cells are tadpole-like structures, less than 0.1 mm long, that are carried to the epididymis for maturation. Epididymis, a long coiled tube, rests on the top and lateral side of each testis. Peristaltic waves in the epididymis help the sperm move into the vas deferens, where the sperm is stored until ejaculation. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 30 Anatomy and Physiology Continued Prostate gland surrounds the urethra at the base of the bladder. It secretes a thin fluid with an alkaline pH that neutralizes the acidic sperm-containing fluid and vaginal secretions to provide an optimal pH for fertilization. Organ of male copulation is the penis, which has a slightly enlarged end, called the glans penis. Male sex hormones are called androgens. Testosterone stimulates the testes to enlarge, increases body hair growth, thickens skin and bone, increases muscle growth, and matures sperm cells. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 31 Male Reproductive Anatomy Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 32 Disorders of the Male Reproductive Tract: Prostatic Diseases Prostatitis—inflammation of prostate usually caused by bacterial infection. Symptoms are dysuria, tenderness of prostate region, secretion of pus. Treatment: antibiotic. Benign prostatic hypertrophy—swelling of prostate gland; partially blocks flow of urine, creating medium for bacterial infection. – Diagnosis: patient complaints and digital rectal examination – Treatment: αlpha-adrenergic blockers to relax smooth muscles; surgical removal of the prostrate gland through a transurethral resection Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 33 Prostate Cancer Common over age 50; second highest cause of cancer deaths in males. Symptoms—urinary obstruction, increased bouts of urinary infection, and frequent nocturia. Digital rectal examination identifies a firm or irregular area. Prostate specific antigen levels increase with presence of cancer. PSA blood test most reliable mass screening test for disease; recommended by age 50 or younger if family history. Treatment: hormone therapy with estrogen; surgical removal of prostate; radioactive seed implantation. Surgical treatment may result in impotence. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 34 Benign Prostatic Hypertrophy and Carcinoma of the Prostate Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 35 Pathologic Conditions Epididymitis—caused by UTI, prostatitis, or an STD. Patients complain of severe low abdominal and testicular pain; swelling and scrotal tenderness. Treat with antibiotics. Balanitis—inflammation of glans penis; occurs most often in uncircumcised patients with narrow foreskins that do not retract easily and in patients with diabetes. – Treatment: antibiotics and cleansing for buildup of smegma Hydrocele—buildup of fluid in the scrotum; may be congenital, acquired because of injury, or age-related. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 36 Tumors of Testes Testicular tumors usually occur in young men and are generally malignant. The patient complains of a hard, painless, mass affecting one testicle. Treatment of the tumors is usually a combination of orchiectomy, radiation therapy, and sometimes chemotherapy. Male patients should be taught testicular selfexamination by the age of 15. See Procedure 39-1. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 37 Impotence and Infertility Impotence is the inability to achieve and maintain an erection sufficient for intercourse. It has many causes, both psychologic and physiologic. This condition can be treated medically with Viagra. Male infertility may be caused by cryptorchidism; varicoceles; low sperm count and motility; obstruction of vas deferens; and hormonal imbalances. – Diagnosis: Examination of semen specimen; sperm count and motility Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 38 Sexually Transmitted Diseases (STDs) There is no cure for viral STDs such as HIV or herpes. STDs are frequently asymptomatic and can cause serious health problems, even death. Genital herpes simplex (HSV-2)—Painful vesicles and ulcers with erythema and pruritus; pain before outbreak; lesions heal in 3 to 4 weeks; may have viral shedding when asymptomatic; dangerous to newborn. Treatment: Zovirax, Valtrex. Genital warts (HPV)—Cause lesions but not always present in infected males; warts tend to recur; may cause cancer of the cervix. Treatment: cryosurgery, creams. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 39 Bacterial STDs Bacterial STDs are increasingly resistant to antibiotics. Gonorrhea and chlamydia—tend to coexist; symptoms similar to acute urethritis and epididymitis. Chlamydia resistant to penicillin, so antibiotics other than penicillin should be used. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 40 Bacterial STDs Syphilis begins with a chancre on the male genitalia within a few days to a few weeks after exposure. Diagnosis: VDRL or RPR blood tests. Goes through six stages if not treated early; can cause death, severe debilitation. Treatment: penicillin G, doxycycline. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 41 HIV and AIDS HIV transmitted by sexual exposure, IV drug use, blood and blood products, infected mother to fetus. Virus invades T lymphocytes, affecting cellular immunity. Initial symptoms flulike—fever, arthralgia, myalgia, lymphadenopathy, rash, night sweats, malaise. Could be at least 10 years before clinical symptoms of AIDS. Greatest increase in incidence—young sexually active women. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 42 AIDS Marked by wide range of opportunistic infections. develop because of low T cell counts. Patient diagnosed with AIDS when T cell count below 200 and/or opportunistic infections diagnosed. – Pneumocystis carinii pneumonia – Candidiasis – Kaposi’s sarcoma – Dementia – Wasting syndrome Treatment: combination of antiviral drugs; cost more than $1000/month; medications must be taken two to three times per day. Current treatment involves postponing development of AIDS. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 43 The Medical Assistant’s Role in Urologic and Male Reproductive Examinations Assisting with a urologic examination – Drape, gown, and position patient – Assist male physicians with female patient examination Assisting with a male reproductive examination – Drape, gown, and position patient – Watch for signs of discomfort and anxiety Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 44 Vasectomy A vasectomy is a surgical procedure for sterilizing a male patient. May be done in the doctor’s office. Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 45 Vasectomy (cont’d) Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 46 Patient Education Male Preventative Medicine By age 50 – Annual physical exam – PSA level and prostate exam – Fecal occult test – Sigmoidoscopy or colonoscopy – Screening for heart disease and diabetes Copyright © 2007 by Saunders, Inc., an imprint of Elsevier Inc. Slide 47