Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
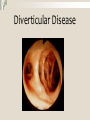
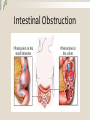
Gastrointestinal Disorders (part 2) N250, Spring 2015 CSULB School of Nursing Inflammatory Bowel Disease (IBD) Immunologic disease that results in idiopathic intestinal inflammation Includes two distinct but similar conditions: Crohn's disease Ulcerative colitis Ulcerative Colitis (UC) Involves chronic inflammation of mucosal and submucosal layers of colon and rectum Begins at base of crypts of Lieberkün; causes congestion and edema leading to ulcers Ulcers bleed easily causing bloody stools Crohn's Disease Can occur in any portion of GI tract Involves all layers of intestinal wall (full thickness disease Usually affects the jejunum and ileum Epidemiology & Manifestations Approximately 1.4 million in the United States have IBD Incidences of Crohn's and UC are similar Men and women affected equally with IBD; higher in Whites UC and Crohn's both have: Abdominal pain, diarrhea, rectal urgency Systemic manifestations Laboratory & Diagnostic Tests Colonoscopy (avoid with severe inflammation) Serologic tests to distinguish between UC and Crohn's disease Two genetic markers have been developed for clinical use Medical Management Eliminate intestinal inflammation Medication and dietary changes is first course Surgery: depends on type of IBD and location and extent of lesions Severe UC: ileal pouch anal anastomosis (IPAA) or continent ileostomy Nursing Management Most managed with medications, dietary changes, and stress reduction Educate patient about medications, stress, diet Suggest support networks Diverticular Disease Diverticular Disease Results from abnormal saclike outpouchings of intestinal wall Can occur anywhere in GI tract except rectum Includes diverticulosis and diverticulitis Diverticular Disease Diverticulosis small, bulging pouches (diverticuli) form inside the lower part of the intestine, usually in the colon. Constipation and straining during bowel movements can worsen the condition. Diverticulitis occurs when the pouches in the colon become infected or inflamed. Pathophysiology, Etiology, and Epidemiology Diverticula form where weak points exist in intestinal wall If a fecalith forms, ischemia and perforation can occur Risk increases with age; particularly after age 60 Clinical Manifestations & Diagnostic Tests Patients are often asymptomatic With exacerbation get left lower quadrant pain, fever, chills Complications are rare Complete blood count (CBC) with differential for bleeding and infection Ultrasonography or CT scan to assess inflammation Medical Management Diet change (high fiber) Rest, drug therapy for mild symptoms IV fluids, IV antibiotics, pain management for more severe symptoms If no improvement in 3 days, bowel resection with anastomosis may be needed Dietary Management High-fiber diet (25 to 30 g daily) to prevent flare-ups 2000 ml of fluid daily (unless contraindicated) When exacerbated (diverticulitis) Clear liquid diet Then low residue (low fiber) diet Resume a high fiber diet when symptoms subside Colon Cancer Colon Cancer Epidemiology and etiology Abnormal cell growth in colon or rectum Only 39% of cases found early Screenings: colonoscopy, double-contrast barium enema, CT colonography (age 50 years) Pathophysiology Risk factors: IBD, family history, increased age, lifestyle factors (diet, smoking, alcohol) Larger the polyp, more likely to be malignant Evidence to a link between C-reactive protein and colon cancer Adenocarcinoma is most common type, accounts for 95% of colon tumors Incidence of colon cancer related to location Clinical Manifestations Usually asymptomatic until it is advanced Symptoms depend on location and of growth Most common symptoms: change in bowel habits or stool texture (Constipation is predominant symptom) Rectal bleeding, hematochezia, passage of red blood via the rectum Anemia Mass in abdomen, Obstruction Laboratory & Diagnostic Tests Hemoglobin and hematocrit values usually decreased Fecal occult blood test Colonoscopy with tissue biopsy CT scan to detect possible metastasis C-reactive protein and carcinoembryonic antigen (CEA): inflammation and as tumor marker Medical/Surgical Management Polypectomy Colectomy Resection Postoperative care includes: Colostomy and wound management Nasogastric tube Colostomy management Wound management Chemotherapy and radiation therapy Nursing Management Early detection is key for prognosis Focus on pre-and postoperative care and support Emotional support is paramount Dietary modifications (give specific information about good/bad food choices) Exercise, reducing obesity Collaborative Management Interdisciplinary team of health care professionals Diagnosis, management, follow-up care Dietary, lifestyle changes, long-term management Stomas and stoma care Colostomy Care Normal appearance of the stoma Signs and symptoms of complications Choice, use, care, and application of appropriate appliance to cover stoma Measures to protect the skin Dietary measures to control gas and odor Resumption of normal activities Interventions for Anticipatory Grieving Observe and identify: Client and family’s current methods of coping Effective sources of support in past crises Client and family’s present methods of coping Signs of anticipatory grieving, such as crying Intestinal Obstruction Intestinal Obstruction Impairment of the forward movement of intestinal contents Mechanical cause Adhesions Tumors Hernias Intussusception, volvulus Functional cause (a.k.a. paralytic ileus) Causes of obstruction Intestinal Obstruction: Etiology and Epidemiology Can occur anywhere from the pylorus to the rectum Can be partial or complete Most bowel obstructions occur in the small intestine Obstructions can be classified by severity, extent, or location Intestinal Obstruction: Etiology and Epidemiology Severity: includes simple or strangulated effects Simple: no impairment of blood or nerves on intestinal wall Strangulated: extremely serious and requires immediate medical attention Pathophysiology Pathophysiology same regardless of cause When obstructed, fluid and gas accumulate Fluid due to inability to reabsorb water Gas due to bacteria and swallowed air Distension can increase risk for pneumonia and atelectasis Clinical Manifestations Most common symptom: cramping or colicky pain that increases Distension Absent or decreased bowel sounds If obstruction in proximal small bowel: vomiting Obstruction in distal small bowel: pain intense; patient may vomit fecal material Laboratory & Diagnostic Tests X-rays, CT scan, complete blood count with differential WBC Barium swallow or barium edema Careful history and physical examination Medical & Surgical Management Relieving obstruction and pressure to avoid perforation Nasogastric (NG) tube used to decompress the bowel Surgery if mechanical obstruction or strangulation Bowel resection Colostomy Bypass procedure Nursing Management Assessment of present condition Instituting fluid and electrolyte replacement Performing bowel decompression via NG tube placement