Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
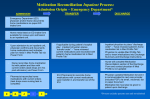
Medication Reconciliation Inpatient Process: Admission Origin–Ambulatory Surgery or Procedural Area* TRANSFER ADMISSION • Ambulatory Surgery or Procedural Area Nurse documents home medications in Med Profile Tab (single shared medication list) via pre-op/preprocedural checklist • Home meds listed in Med Profile tab are available for screening against medications to be administered during procedure/surgery • Post-operatively, inpatient physician confirms home medications and indicates plan for meds in Med Profile Tab via Power Form • • D • If applicable during patient’s hospital stay: inpatient physician places “transfer order” – “have reviewed current medications and reconciled with patient’s home medication list in Med Profile Tab” Nurse reconciles home medication list with patient and then with current orders (task drops at 4 hrs post admission) via Power Form Pharmacist reconciles home medications with current orders (task drops once nursing task is complete) M A I C • ICU pharmacist to reconcile home medications with current medications upon transfer in and transfer out of the ICU DISCHARGE • • Inpatient physician to place “discharge order” – “have reviewed patient’s home medication list in Med Profile Tab” Physician to update Med Profile Tab and to insert medications into Discharge Summary and Discharge Instructions • Nurse will complete Medication Reconciliation section of the Discharge Form and contact physician if Med Profile is not updated • Physician updates Medication list and it is communicated to next care provider (includes PCP) via email, voicemail, fax or paper document Medication list must also be given to patient upon discharge • *Process excludes patients seen and not admitted