Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Compartmental models in epidemiology wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Diseases of poverty wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Seven Countries Study wikipedia , lookup
Epidemiology wikipedia , lookup
Public health genomics wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
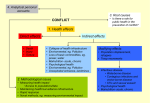
ICD-10 Preparation: Understanding your own data to create your ICD10 Strategy for Success Data Analytics and Audit Barbara Godbey-Miller, RHIA, CCS, CHC Today’s Agenda • Step 1: Data Analytics: – Aggregate information analysis • Step 2: Audit Findings – Real results from clients • Step 3: Education – What your team needs to know But First A Word About Data Governance and Clinical Documentation Integrity Data Variables Physician Clinical Clinical Documentation Documentation Program Understanding the clinical documentation specificity of I-9, a system used for 30 years, required a CDI program to manage. What will the CDI error rate be? Managing the I-10 CDI process will require additional staff to cover increased workload. Will staffing be adequate to cover 100% of cases & what percentage of queries will go unasked or unanswered? Coding Accuracy ICD-10 coder errors will increase with use of new system and increased requirement to interpret physician documentation requirements. What will the coding error rate be of coders and contract personnel? Coding Quality Review With increase demand for coding resources and cash flow demands, will organizations have an internal coding quality review process to identify increased coding errors? Regulatory Data Normalization Change Not all DRGs are created equal or have the same probability for DRG assignments errors. Data normalization without manipulation. What is your DRG risk population for change and what is the revenue impact? CMS givith and take it away. Regulatory factors should be included to determine revenue impact. • Documentation & Coding Adjustment Factor • Prospective Payment System Changes • ICD-10 Oncology Grouper Changes Clinical Documentation Integrity The HIM professional’s role is to combine emerging technologies with innovative processes to meet the aims of this strategy ─ improve the quality of healthcare, improve the health of the US population, and reduce the cost of quality healthcare. What is Data Governance? Making strategic and effective decisions regarding the organization’s information assets. Includes: – Defining roles and responsibilities for data – Establishing data quality policies – Creating metadata management practices – Arbitrating shared data questions – Release of Information The HIM Professional’s Key to Successful Information Governance • Data or Information governance is the high-level, corporate, or enterprise policies or strategies that define the purpose for collecting data, ownership of data, and intended use of data. Accountability and responsibility flow from governance. • The Information Governance plan is the framework for the overall organizational approach to data governance. Clinical Documentation Integrity The HIM professional’s role is to combine emerging technologies with innovative processes to meet the aims of this strategy ─ improve the quality of healthcare, improve the health of the US population, and reduce the cost of quality healthcare. ICD-10 Analytics Approach Initiate Define assessment scope Identify stakeholders Assess ICD-10 revenue impact analysis Documentation audit Recommend Recommended remediation or mitigation of risk Educational mapping Plan Key activities and timing Put plan into action Focus on highrisk MS-DRGs ICD-10 Data Analytics ICD-10 analytics are derived or analyzed using the GEMS file, which without audit is not a reliable tool to identify DRG shifts ICD-10 Data Analysis Challenges Data Variables GEM mappings There are defined data provide all possible variables that when iterations of ICD-10 applied to a set of codes. Some are very specific assumptions, unlikely. We’ve will provide a more learned from these relevant outcomes wild goose chases. analysis. ICD-10 data analytics will return higher probability rates if they are fact based using a set of variables that will influence the outcomes analysis for DRG assignment predictability Use What We've Learned We’ve found common (40 projects) coding issues causing CC/MCC loss or gain and DRG shifts due to root operations and coding guidelines. Next Steps Prepare an action plan for your hospital based on your risks and our experience. Data Analytics – How its Done • 12 months of claims are processed through an analytics program for ICD-10 CM/PCS using GEMS and reimbursement maps • Data Analysts review each mapping to identify legitimate risks – Two scenarios – financial risk, operational risk • ICD-10 Auditors validate documentation on highest risk areas – Output – Physician and Coder education strategy Data Analytic Analysis 2 Sites - Post Audit Results Total Cases I-9 CMI I-10 CMI 98 1.84 1.56 CMI Increases I-9 CMI I-10 CMI 40 1.31 1.99 CMI Decreases I-9 CMI I-10 CMI 58 2.21 1.27 Post Audit Findings Reason for DRG Change PDX Change Cases 19 Add CC 6 Add MCC 3 Minus CC 15 Minus MCC Root PX DRG Logic 5 56 5 Scenarios Specific examples of MS-DRG changes discovered on I-10 re-code projects MS-DRG SHIFT Cardiology: Patient was readmitted for treatment of post infarction angina & CAD, 1 week status post acute myocardial infarction 303 - Atherosclerosis without MCC RW 0.6034 282 - Acute Myocardial Infarction, Discharged Alive without CC/MCC RW 0.7551 Relative Weight GAIN 0.1517 ICD-10 Re-Code: What We Discovered • MS-DRG changed due to timeframe established within ICD10 to indicate an acute myocardial infarction – Even as a secondary diagnosis, the AMI will “drive” this MSDRG based on grouper logic with PDX from Circulatory MDC 5 and AMI • Category I21 (AMI) is coded up to 4 weeks following the AMI regardless of reason for admission • The terminology used in ICD-9 to capture “subsequent episode of care” for AMI does not exist in ICD-10 – Subsequent AMI codes are used when a patient has a second AMI within 4 weeks of the initial AMI – NOTE: “Subsequent” refers to the MI and NOT the episode of care in ICD-10 Acute Myocardial Infarction • ICD-10-CM has decreased the acute phase of an acute myocardial infarction from 8 weeks or less to 4 weeks (28 days) or less. • ICD-10-CM classifies acute myocardial infarction in two separate categories. STEMI and NSTEMI • Clinical documentation will need to indicate laterality. Additional specificity is required to identify the anatomical site affected I21.02 ST elevation (STEMI) myocardial infarction involving left main coronary artery Laterality Subsequent Myocardial Infarction • • • ICD-10-CM has added a category for subsequent myocardial infarction. Subsequent is identified as a myocardial infarction occurring within 4 weeks (28 days) of a previous myocardial infarction. Clinical documentation must include the type of subsequent myocardial infarction Example: A patient is admitted with a subsequent STEMI of the anterior wall 7 days after being discharged for a STEMI of left main artery, anterior wall Code indicates this is the subsequent MI I22.0 subsequent STEMI myocardial infarction of anterior wall I21.01 STEMI myocardial infarction involving left main coronary artery of anterior wall Code indicates this was the first MI Potential Readmission Flag ICD-9 Acute Myocardial Infarction – 8 weeks ICD-10 Acute Myocardial Infarction – 4 weeks Readmission Risk if patient winds up back in the hospital in 30 days. Zero additional payment – potential gain may be lost in this instance MS-DRG SHIFT Cardiology: Patient was admitted with AMI and had coronary intervention with four drug-eluting stents. 246 – Percutaneous Cardiovascular Procedures with drug-eluting stent w/MCC OR 4+ vessels/stents RW 3.1830 247 - Percutaneous Cardiovascular Procedures with drug-eluting stent without MCC RW 2.0408 Relative Weight LOSS 1.1422 ICD-10 Re-Code: What We Discovered • MS-DRG changed due to the fact that even though patient had four drugeluting stents inserted there were only three sites being treated • In ICD-10- PCS, the code is assigned based on number of sites being treated rather than number of stents inserted • Occasionally, this will result in lowerweighted DRG assignment in ICD-10 Documenting Procedures • Clinical documentation for all procedures will require documentation identifying the following: General physiological system or anatomical region involved Body system Rootoperation Operation administration, dilation, drainage, biopsy, What type of procedure was performed root excision, resection, bypass, transplantation The exact anatomical site of the procedure body partBody part Right, left, bilateral Laterality The technique used to reach the site surgical Surgical appro approachach open, closed, laparoscopic, percutaneous, endoscopic, needle If a devDevice ice was used, what site/area was the device placed (e.g. stent, graft, implant) If the procedure was for diagnostic purposes Qualifier Documenting Procedures • When a PTCA is performed, clinical documentation by the physician must indicate how many sites were dilated and what device was utilized for “each” site. Example: OR report indicates that patient had PTCA of both the left anterior descending artery and the right coronary artery. A drug-eluting stent was placed in the right coronary artery. No stent inserted 02703ZZ Dilation, Artery, Coronary, One Site 027034Z Dilation, Artery, Coronary, One Site Stent inserted Two codes required to identify procedure on each artery MS-DRG SHIFT Medicine: Patient was admitted for treatment of anemia secondary to ESRD. Patient also has hypertension. 811 - Red Blood Cell Disorders with MCC RW 1.2488 682 – Renal Failure with MCC Relative Weight GAIN RW 1.5401 0.2913 ICD-10 Re-Code: What We Discovered • MS-DRG changed due to change in principal diagnosis per sequencing instructions in ICD-10CM Official Coding Guidelines • Anemia in chronic kidney disease is a classified as a manifestation of chronic kidney disease – Manifestation codes cannot be assigned as principal diagnosis • Notes instruct to code first the underlying disease of ESRD • Under ESRD, there is another instructional to code first any hypertensive chronic kidney disease Chronic Kidney Disease ICD-10-CM uses the following table to identify the stage of kidney disease Chronic Kidney Disease Severity Stages Stage 1 Stage 2 (mild) Stage 3 (moderate) Stage 4 (severe) Stage 5 End stage renal disease Chronic kidney disease, unspecified Hypertensive Diseases • Clinical documentation for hypertension in ICD-10CM should be described as accelerated, benign, essential, idiopathic, malignant, and systemic Documentation by physician indicates Essential I10Essential (primary) hypertension Hypertensive Diseases • ICD-10-CM presumes a cause-and-effect relationship between hypertension and chronic kidney disease. Clinical documentation will need to include the stage of chronic kidney disease. Clinical documentation indicates hypertension and chronic kidney disease I12 N18.5 Hypertensive Kidney Disease Chronic Kidney Disease, Stage 5 Clinical documentation requires the correct staging of the chronic kidney diseases Hypertensive Diseases Example: A 68-year-old gentleman is admitted with hypertension, heart disease, acute on chronic CHF, and stage 4 renal disease. The physician documents that the heart disease is associated with the hypertension. Code shows hypertension, heart disease, CHF, and stage 4 renal disease all combined in one code I13.10 N18.4 I50.33 Hypertensive heart and chronic kidney disease with heart failure, with stage I-IV CKD Additional codes show stage of Chronic Kidney Disease, Stage 4, severe Acute on chronic diastolic heart failure CKD and specificity of heart failure Chronic Kidney Disease with Hypertension • ICD-10-CM presumes a relationship between chronic kidney disease and hypertension. Disease • Clinical documentation for hypertensive kidney disease will also require identification of the stage of Stage of CKD kidney failure I12 Hypertensive Kidney Disease N18.5 Chronic Kidney Disease, Stage 5 Hypertensive Heart and CKD Case Study A 68-year-old gentleman is admitted with hypertension, heart disease, acute on chronic CHF, and stage 4 renal disease. The physician documents that the heart disease is associated with the hypertension. Disease I13.10 Hypertensive heart and chronic kidney disease with heart failure, with stage I-IV CKD N18.4 Chronic Kidney Disease, Stage 4, severe I50.33 Acute on chronic diastolic heart failure Stage of CKD Type of Heart Failure MS-DRG SHIFT Medicine: Patient was admitted for treatment of anemia secondary to lung cancer 812 - Red Blood Cell Disorders without MCC 182 – Respiratory Neoplasms without CC/MCC RW 0.7985 RW 0.8275 Relative Weight GAIN 0.029 ICD-10 Re-Code: What We Discovered • MS-DRG changed due to change in principal diagnosis per sequencing instructions in ICD-10-CM Official Coding Guidelines • When the admission is for management of an anemia associated with malignancy, and the treatment is only for anemia, the appropriate code for the malignancy is sequenced as the principal or first-listed diagnosis followed by code D63.0, Anemia in neoplastic disease Anemia in Chronic Diseases • ICD-10-CM classifies anemia in chronic diseases into several categories. Clinical documentation will be required to identify the type of chronic anemia as well as the associated cause Anemia in neoplastic disease Documentation will need be required to identify associated neoplasm Anemia in chronic kidney disease Documentation will be required to identify the stage of chronic kidney disease Acquired Aplastic Anemia • Clinical documentation for acquired aplastic anemia should indicate the cause as follows: High-dose radiation or chemotherapy Environmental toxins Medications Viral infections Autoimmune disease Paroxysmal nocturnal hemoglobinuria MS-DRG SHIFT Surgery: Patient was admitted with rectal bleeding and peritoneal abscess. Treatment included partial resection of ileum and lysis of peritoneal adhesions. 329 – Major small and large bowel procedures with MCC RW 5.1272 335 – Peritoneal adhesiolysis with MCC RW 4.1615 Relative Weight LOSS 0.9657 ICD-10 Re-Code: What We Discovered • MS-DRG changed due to the fact that a partial small bowel resection (ileum in this case) no longer groups to major small and large bowel procedures DRG in ICD-10 • Surgical hierarchy dictates the principal procedure selection – In this case, the lysis of adhesions overrides any other procedure performed based on surgical hierarchy MS-DRG SHIFT Pulmonary: Patient was admitted with exacerbation of COPD. Patient also had accelerated hypertension which was treated. 191 – COPD with CC RW 0.9343 192 – COPD without CC/MCC Relative Weight LOSS RW 0.7120 0.2223 ICD-10 Re-Code: What We Discovered • MS-DRG changed due to the fact that a specific code for accelerated or malignant hypertension does not exist in ICD-10 thereby, eliminating the ability to capture CC • There is only one code for hypertension in ICD-10 which encompasses all types and is NOT classified as a CC Diseases of the Gastroenterology System • Clinical terminology used to describe diseases of the digestive system and has been updated to reflect advances in diagnosis and procedures as well as greater specificity Example: ICD-9-CM 555.1 Regional enteritis large intestine ICD10-CM K50.10 Crohn’s disease of large intestine without complications K50.111 Crohn’s disease of large intestine with rectal bleeding K50.112 Crohn’s disease of large intestine with intestinal obstruction K50.113 Crohn’s disease of large intestine with fistula K50.114 Crohn’s disease of large intestine with abscess K50.118 Crohn’s disease of large intestine with other complication K50.119 Crohn’s disease of large intestine with unspecified complications Diseases of the Digestive System • Terminology for many of the categories in gastroenterology have been updated to reflect current terminology. • The gastroenterology category contains specific respiratory diagnosis codes for infections, inflammations, causative organisms, and external agents • The physician will be required to document details such as Specific forms of the disease Site of the disease/disorder Laterality Causative organism External agents Associated conditions Acuity Additional Documentation for Gastroenterology • ICD-10-CM requires additional documentation to identify external factors attributing to diagnoses within this category. Clinical documentation will be required to show associated causes such as: Alcohol abuse and dependence Exposure to environmental tobacco smoke Exposure to tobacco smoke in the perinatal period History of tobacco use Occupational exposure to environmental tobacco smoke Tobacco dependence Tobacco use Regional Enteritis (Crohn’s Disease) • ICD-10-CM categorizes regional enteritis (Crohn’s Disease) by site: Small intestine Large intestine Both small and large intestine • Clinical documentation will also be required to identify any associated complications such as: Abscess Fistula Intestinal obstruction Rectal bleeding Other specified complication K50.114 Crohn’s disease of large intestine with abscess Disease Location Complication Ulcerative Colitis • Clinical documentation for ulcerative colitis in ICD-10-CM will require identification of the site of ulcerative colitis or other condition within this category, such as: • Inflammatory polyps Left sided colitis Panocolitis (enterocolitis, ileocolitis, universal colitis) Proctitis Rectosigmoiditis (proctosigmoiditis) Other specified site Additional documentation will be required to identify any associated complication, such as: Abscess Fistula Intestinal obstruction Rectal bleeding Other specified complication Diverticulosis/Diverticulitis • Clinical documentation will be required to identify between diverticulosis and diverticulitis • Specificity will be required to identify the location of the disease as: Small intestine Large intestine Both small and large intestine • Additional documentation will be required to identify any associated conditions such as: Perforation Abscess Bleeding Disease Location No associated conditions K57.32 Diverticulitis, large intestine, without perforation or abscess, without bleeding Diagnosis Quick Tip Barrett’s Esophagus With dysplasia - Low grade - High grade Without dysplasia Gastritis Acute, alcoholic, chronic superficial, chronic atrophic, associated hemorrhage Gastroenteritis Salmonella, viral, infectious, toxic, allergic, causative agents, causative organism Alcoholic liver disease Alcoholic fatty liver, alcoholic hepatitis, alcoholic fibrosis and sclerosis of liver, alcoholic cirrhosis liver, alcoholic hepatic failure, associated ascites, associated coma Acute Pancreatitis Alcohol-induced, biliary (gallstone), drug induced, idiopathic Documenting Procedures • Clinical documentation for all procedures will require documentation identifying the following: General physiological system or anatomical region involved Body system Root Operation administration, dilation, drainage, What type of procedure was performed root operation biopsy, excision, resection, bypass, transplantation Body part The exact anatomical site of the procedure body part Right, left, bilateral Laterality The technique used to reach the site surgical a open, closed, laparoscopic, Surgical approach percutaneous, endoscopic, needle If a d Deviceevicwas used, what site/area was the device placed (e.g. stent, graft, implant) If the procedure was for diagnostic purposes Qualifier Partial Large Bowel Resection Operating Room Report indicates open right hemicolectomy with end-to-end anastomosis for treatment of large carcinoid tumor Large Intestine, Right No Device ODT F 0 Z Z Resection Open Approach No Device Chronic Obstructive Pulmonary Disease • The following conditions are classified in this category: Asthma with chronic obstructive pulmonary disease Chronic asthmatic (obstructive) bronchitis Chronic bronchitis with airways obstruction Chronic bronchitis with emphysema Chronic emphysematous bronchitis Chronic obstructive asthma Chronic obstructive tracheobronchitis • Clinical documentation of chronic obstructive pulmonary disease should identify any associated acute exacerbation or lower respiratory infection Disease J44.0 Chronic obstructive pulmonary disease with acute lower respiratory infection J20.2 Acute bronchitis due to streptococcus Associated Condition/Organism Emphysema • Clinical documentation for emphysema should include a full description of the disease and document the specific types as: Unilateral emphysema (MacLeod’s syndrome) Centrilobular emphysema Panlobular emphysema Other emphysema Unspecified emphysema • Clinical documentation should also include any associated exposures such as: Exposure to environmental tobacco smoke History of tobacco use Occupational exposure to environmental tobacco smoke Tobacco dependence Tobacco use Asthma • Clinical documentation should identify additional diagnoses that could affect the current treatment of asthma, such as: Exposure to environmental tobacco smoke Exposure to tobacco smoke in the prenatal period History of tobacco use Occupational exposure to environmental tobacco smoke Tobacco dependence Tobacco use Allergen induced Exercise induced Stress induced Associated respiratory infections • Additional documentation should identify the long term use of steroids associated with asthma: Long term (current) use of inhaled steroids Long term (current) use of systemic steroids Asthma • Clinical documentation will require specificity to show whether the reported asthma is “uncomplicated”, “with acute exacerbation”, or “with status asthmaticus” • Clinical documentation of asthma should always include the following: Acute exacerbation of asthma With status asthmaticus Type of asthma Mild Intermittent Persistent Moderate persistent Severe persistent Other specified type Unspecified type Intrinsic (nonallergic) Extrinsic (allergic) Associated external agents Asthma • Clinical documentation should identify Asthma of Daytime Symptoms theSeverity severity of Frequency asthma Intermittent Less than or equal to 2 times per week Mild Persistent More than 2 times per week Moderate Persistent Daily. May restrict physical activity Severe Persistent Throughout the day. Frequent severe attacks limiting ability to breathe. Asthma Case Study 40-year-old female presents with a diagnosis of acute asthma. She has a long history of moderate persistent asthma. She takes inhaled steroids daily. Final discharge diagnosis is documented as moderate persistent asthma with acute exacerbation. Severity J45.41 Acuity Moderate persistent asthma with (acute) exacerbation Z79.51 Long term (current) use of inhaled steroids Use of Steroids Respiratory System Documentation Diagnosis Quick Tip Pneumonia Causative Organism, manifestation of other condition, lobar, multilobar COPD Associated acute respiratory infection, acute exacerbation, Causative agents, long term use steroids Influenza Type, causative organism, manifestations Asthma Type, intermittent, persistent, mild, moderate, severe, causative irritant, exacerbation, associated conditions, status asthmaticus Respiratory Failure Acute, chronic, with hypoxia, with hypercapnia, Associated conditions, causative irritants In Summary: Clinical Documentation Integrity • Integrity of health information is an obligation of HIM • HIM professionals must assume a leadership role in transforming these functions • Now is the time to analyze and visualize documented and undocumented intra and interdepartmental HIM functions to understand the current and future state of the HIM department while ensuring HIM best practices and standards are consistently maintained Action Items as you prepare for ICD10 Implementation – Identify risks and opportunities for your hospital – Use examples in this presentation to identify the same issues in your facility • DRG Shifts – Positive » Principal Diagnosis » Principal Procedure (root operation) » CC/MCC – Negative » Principal Diagnosis » Principal Procedure (root operation) » CC/MCC – Educate Physicians, CDI Team and Coding Professionals – Compare I-9 to I-10 DRG assignment if dual coding Action Items post - Implementation – Prepare a DRG report by month for beginning the go live date • List of cases by individual DRG – Compare by month DRGs year to year • Identify total numbers for pre-I-10 and post I-10 by DRG for each month • Work the list of DRG shifts – Print out I-9 DX and PX with descriptions – Compare to I-10 DX and PX with descriptions – Identify PDX, PPX and CC/MCC changes