Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
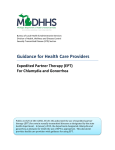
Expedited Partner Therapy: Background & Current Status Matthew Hogben PhD Centers for Disease Control and Prevention (404) 639-1833 [email protected] February 9, 2010 The findings and conclusions in this presentation are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention Overview Context and Background Expedited partner therapy (EPT) definition and principles Historical use of EPT Evidence of EPT efficacy and effectiveness RCT results: index patient reinfection and behavior Composite estimates Implementation of EPT as a strategic option Core requirements and coverage issues Barriers Implementation progress Next steps 2 Partner Referral Approaches No Public Health Involvement Required Nothing Public Health Involvement Required Provider referral Self referral or patient referral Patient is intended to notify partners of exposure (with varying levels of provider encouragement) A public health professional elicits partners’ identifying information and contacts and notifies partners Contract or conditional referral Patient gets initial chance to contact and notify partners, but professional will do so if patients do not (within a specified time frame) 3 Historical PN “Contact tracing” Even in the absence of therapy, useful for interrupting transmission (1930s) In conjunction with therapy, rapid drop in syphilis (1940s and 1950s) Conducted largely by trained public health staff Seems to work for syphilis between 1945 - 1965 4 Piling on the work… Wigfield. Brit J Ven Dis 1972. 5 Case reports per 100,000 (US) 450 400 350 300 2006 2007 2008 250 200 150 100 50 0 Syphilis Gonorrhea Chlamydia STD Surveillance Report (2009), Tables 3, 13, 25. http://www.cdc.gov/std/stats08/toc.htm 6 www.cdc.gov/nchhstp/partners 7 Tailored tactics for different diseases All New HIV (contract) Early Syphilis (provider) Repeat GC (provider) All STD clinic-based GC Follow-up Interview FDT Internet Notification Other GC, All CT (EPT) Re-interview subset Using all those evaluation $$ One of multiple possible program approaches to PN 8 Definition and Principles Questions so far? Expedited Partner Therapy Core elements A STD that is treatable via oral medication A point of origin in which medications or prescriptions can be disbursed A mechanism through which either can be brought to sex partners of infected people CDC. Expedited partner therapy. 2006 10 EPT Referral Strategies Basic Strategy (1) Patient referral or self referral (1) PDPT Patient is intended to notify partners of exposure (with varying levels of provider encouragement) (2) Provider referral EPT “addition” Provider (meaning public health staff as default) is intended to notify partners of exposure Patient carries prescription or medication for partner along with instructions (2) Field-delivered therapy Provider notifies and delivers prescription or medication (plus instructions, etc.) 11 Historical use: 1999 to present Several local surveys and one national survey Across estimates: widespread, not common At least half of respondents (physicians, nurse practitioners) had used PDPT at least once Approximately 11 – 15% used PDPT “frequently” Usually or always (National survey) 74 – 100% of patients (Seattle, WA) Larger proportions in CA (>40% routinely) and NYC (25%+) 12 NEJM 1977 13 Efficacy and Effectiveness Questions so far? Establishing Efficacy: Key Outcomes Effect on clinically relevant outcomes establishes EPT efficacy Index patient reinfection rates Treatment rates Notification rates Patient and partner behaviors Collateral benefits or harms These are the same outcomes by which one would judge any PN intervention or program 15 Reinfection rates IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII Trelle et al. BMJ 2007. 16 Treatment rates Trelle et al. BMJ 2007 17 GC and CT outcomes (Seattle) Gonorrhea 6 of 179 (EPT) 19 of 179 (Control) RR = 0.32 (0.13 – 0.77) Chlamydial infection 86 of 797 (EPT) 105 of 798 (Control) RR = 0.82 (0.62 – 1.07) Note the similarity to the 6-city RCT: These are probably minimum effect sizes 18 Patient and Partner Behaviors 19 CDC Guidance From the 2006 Review and Guidance http://www.cdc.gov/std/ept/default.htm See also: 2006 STD Treatment Guidelines http://www.cdc.gov/std/treatment/ 2008 Recommendations for Integrated Partner Services http://www.cdc.gov/nchhstp/partners/ 20 Guidance for Use of EPT Heterosexual males and females Gonorrhea and chlamydial infection Accompany with written instructions Men who have sex with men How to take meds, allergies, seek evaluation More caution (fewer data, more HIV comorbidity) Trichomoniasis, syphilis Much more caution, “last resort” 21 Implementation Questions so far? Prevention Impact framework Efficacy or effectiveness (in targeted groups) Contribution of groups to population health outcome X = X Effective level of coverage PREVENTION IMPACT Abridged/adapted from: Aral et al. Behavioral Interventions 2007; St. Louis & Holmes Sexually Transmitted Diseases (3rd ed.). 1999 23 Achieving impact with EPT EFFICACY Tx rate: 20% To 100% increase Reinfection: 20% to 50% decrease CONTRIBUTION X Partners have 20% to 75% positivity (program data) X COVERAGE Key Issue 24 Patients and Physicians Discuss PDPT Probable maximum effect, balanced by reduced coverage 25 Core elements A STD that is treatable via oral medication GC and CT in this case A point of origin in which medications or prescriptions can be disbursed A mechanism through which either can be brought to sex partners of infected people Barriers to coverage: What gets in the way? 26 Those Barriers to Coverage Not sure how to get started logistically Discomfort with no health provider face to face contact with partner Legal landscape in jurisdiction Costs 27 Protocols and other resources 28 Some PH contact: Field-delivered therapy Steiner AJPH 2003 29 30 Legal landscape Basic legal inhibitions center around Prescribing rules, dispensing rules, established patient relationship Review of legality Yields a spreadsheet with facilitators and barriers in laws, regulations, policy statements, AG statements, judicial rulings Published as a website – “The information presented here is not legal advice, nor is it a comprehensive analysis of all the legal provisions that could implicate the legality of EPT in a given jurisdiction.” 31 “Legal” implementation advice Explicit endorsement through laws Create exceptions to existing prescription requirements Increase professional board and association support Facilitate 3rd party payment 32 Has coverage increased? 2006 10 states had express legislation/permission (3) or other legal conditions not prohibiting the practice (7) 13 had clear legal conditions prohibiting the practice (not aimed at EPT specifically) The remainder had no clear position one way or another 2010 The corresponding numbers are 23 (+ Baltimore), 8, and 19 (- Baltimore) 33 Evolving Landscape of EPT: Legal Status Summary WA VT MT ND ME MN OR ID WI SD IL UT RI WV KS AZ VA CT KY NC TN OK NM AK MO A R MS AL EPT is Permissible NJ SC DE GA EPT is Likely Prohibited MD LA TX 2006 MA OH IN CO CA NH PA IA NB NV NY MI WY DC FL EPT is Potentially Allowable HI Legislation Pending WA VT MT ND ME MN OR ID WI SD PA IA NB NV IL UT NY MI WY RI WV KS AZ OK NM AK MO VA KY NC TN A R SC MS TX AL GA LA FL HI 2010 MA OH IN CO CA NH CT NJ DE MD DC (Baltimore only) Baltimore implementation Implementation (as of Jan 2009) STD clinics Medications dispensed GC/CT, 3 extra dose maximum Evaluation Uptake = 1046/1533 (68%) Modal extra doses: women = 1; men = 2 Active assessment of adverse events in STD clinics + passive reporting from other providers No adverse events (again) Repeat infection rate = 2.3% in 2008 (compared to 3.9% in 2007 w/o EPT, p = .10) 41% reduction, has been further followed up 35 Next Steps Questions so far? Current and near future (selected) Toolkit: Needs assessment to inform content for states interested in legal provisions and subsequent policies Incorporation into Best Practices Engagement with other federal agencies (CMS) National CT Coalition support Effectiveness rating Possible USPSTF review 37 The bigger picture: Shifting furniture It looks heavy Let’s send Mr. Screening to move it Bother. Let’s give Mr. PN a go Fine. Mr. Behavioral Interventions? Um, Mr. EPT? Oh well. 38 All together now… Intervention Mix Along Continuum of Services Efficacy Screening/Testing Patient Treatment Partner Notification & Treatment Counseling and other Interventions Follow-up Care Contribution X STD clinic Other public sector Private sector Coverage X Something for everyone 39 Contact information Matthew Hogben (404) 639-1833 [email protected] 40