Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
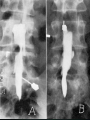
اسكوليوز تعريف اسكوليوز انحراف جانبي ستون فقرات علل ايديوپاتيك نوروماسكوالر مادرزادي نوروفيبروماتوز بيماريهاي مزانشيمي (مارفان “ اهلر دانلوس “ ) ارتريت روماتويد نوجوانان تروما (شكستگي ,بدنبال المينكتومي ,توراكوپالستي ) استوكوندروديستروفيها ( دوارفيسم ,استوژنز ايمپرفكتا , اكوندروپالزي ) ادامه علل عفونت بيماريهاي متابوليك ( دوارفيسم ,هوموسيستونوري ) پره واالنس و شيوع جنسي 3-2 درصد هرچه درجه قوس باالتر باشد در دخترها شايع تر است و به 4برابر ميرسد . ارث Scoliosis Is a single gen disorder .? Natural history . درصد باالتر است100 مرگ و مير درمان نشده ها . شايع ترين علت مرگ كورپولمونال است Nachemson : 130 pat. For 38 years found that 100% more mortality according to general population (16 from 20 mortality was due to corpulmonal , 37% LBP , only 3 pat. Were idioscoliosis . ايا مرگ زودرس داريم ؟ داريم ,ولي در ايديواسكوليوز نداريم . كمر درد در اسكوليوزها ؟ انسيدانس در جمعيت عمومي %60-80است . در اسكوليوزها % 86است . البته شيوع درد روزانه در اسكوليوزها شايعتر از جمعيت عمومي است . در قوسهاي لومبار و توراكولومباردرد كمر شايعتر است . شدت درد با شدت قوس ارتباطي ندارد . ارتروز در راديوگرافي اسكوليوزها با افزايش سن به %90 ميرسد . فونكسيون ريه فقط در قوسهاي توراسيك ارتباط مستقيم دارد . سيگار و hypokyphosisبا عملكرد ريه ارتباط دارد . حاملگي مشخص نيست كه حاملگي موجب افزايش شدت قوس شود .ولي توصيه شده حاملگي زير 20سالگي رخ ندهد . در قوسهاي متوسط انديكاسيون سزارين نمى باشد . ) ترمينولوژي(اصطالحات Cervical curve : apex between C1 & C6 cervicothoracic curve :apex between C7 & T1 thoracic curve :apex between T2 & T11 thoracolumbar curve :apex between t12 & L1 Lumbar curve :apex between L2& L4 بررسي و معاينه معاينه پوست (برهنه ) تست خم شدن به جلو درد web گردني در سندرم ترنر ,كاو عميق در سندرم مارفان ,بزرگي كبد و طحال در موكوپلي ساكاريدوزها . معاينه بلوغ School screening test 14-10 سالگي روش تست . حساسيت تست %100 : اختصاصي تست 45 % : راديوگرافي – APاولين به صورت APاست .ايستاده و گاهي نشسته , – حافظ گنادها بجز در اولين راديوگرافي بكار ميرود . – گرافي الترال هم بصورت ايستاده است . گرافي apايستاده گرافي الترال اثر راديوگرافي بر بافتها پستان ,مغز استخوان ,گنادها ,تيرويد ) AP or PA (5-10 درمان اسكوليوز تحريك الكتريكي تحت نظر ارتوز عمل جراحي تحريك الكتريكي امروزه ديگر انديكاسيون ندارد . بعضي تنها مورد انرا در بيماران نيازمند بريس ميدانند كه بدليلي امكان استفاده از بريس ندارند . observation در قوسهاي زير 20درجه كاربرد دارد . قوسهاي زير 20در سنين كودكي هر 12-6ماه گرافي AP قوسهاي زير 20در سنين نوجواني هر 4-3ماه گرافي AP قوسهاي زير 20در سنين بعد از بلوغ احتياج به اقدام خاص ندارد . بريس قوسهاي 29-20درجه اي كه پيشرفت داشته باشند 5(.درجه در طي 6ماه ) قوسهاي 30-45در اولين برخورد . پيش نيازهاي ارتوز : -1حداقل 12ماه از رشد اسكلتي مانده باشد . -2ريسر 3يا كمتر باشد -3رينگ اپوقيزي باز ياشد . -4بيش از 6ماه از منارك نگذشته باشد . كونتراانديكاسيونهاي بريس بلوغ اسكلتي لوردوز توراسيك قوس باالي 45درجه انواع بريس هرني ديسكال اناتومي تغذيه ديسك فاقد عروق خوني است . از طريق بخش متخلخل مركزي end plateبه روش انتشار تغذيه ميگردد . تغيرات مفاصل فاست طي عمر مرحله ) dysfunction( : 1پارگي حلقوي ديسك سينوويت و هيپرموبيليته مفصل فاست (.) 15-45 مرحله ) instablity( : 2پارگي پيشرونده ديسك , تخريب مفصل فاست و سابلوكساسيون ان 35-70(. )سالگي. مرحله ) stablization( : 3هيپرتروفي اطراف مفصل و انكيلوز كمري (.باالي 60سالگي ) محل شايع دژنرسانس ديسك L4-L5 & L3-L4 عاليم باليني هرني ديسكال درد كمريا گردن ,مشخصات درد درد تير كشنده به ساق اسپاسم عصالت كمري اختالل حسي و حركتي اختالل رفلكس عصبي SLR ريسك فاكتورهاي LBP شغل سنگين كار روي وسايط نقليه سيگارت زايمان زياد قد باالي 180 وزن باال شغل همراه استرس عاليم ديسك گردني عاليم مربوط به خود مهره ,از طريق اعصاب sinovertebralبصورت درد گردني و مديال به اسكاپوال و شانه . عاليم مربوط به فشار به ريشه عصبي . عاليم مربوط به ميولوپاتي كه با lermit signدر MS افتراق ميابد (.در ديسكهاي مياني مشاهده ميشود ). IMAGING IN LOW BACK PAIN Plain Radiographs (X-Rays) Generally not recommended in the first month of symptoms in the absence of “red flags”. The main purpose of plain x-ray is to detect serious underlying structural or pathologic conditions. RED FLAGS (POSSIBLE FRACTURE) Major trauma,such as vehicle accident or fall from height Minor trauma or even strenuous lifting (in older or potentially osteoporotic patient) RED FLAGS (POSSIBLE TUMOR OR INFECTION) Age over 50 or under 20,history of cancer Constitutional symptoms,such as recent fever or chills or unexplained weight loss Risk factors for spinal infection:recent bacterial infection(U.T.I),IV drug abuse,or immunesuppression(from steroids,transplant or HIV) Pain that worsen when supine,severe nighttime pain RED FLAGS (POSSIBLE CAUDA EQUINA SYN.) Saddle anesthesia Recent onset of bladder dysfunction: (retention,frequency,overflow incontinence) Severe or progressive neurological deficit in lower extremity Anal sphincter laxity,perineal sensory loss Major motor weakness:quadriceps,ankle plantar flexors,evertors, and dorsiflexors (foot drop) OBLIQUE VIEWS Are rarely indicated and increase both the cost and radiation exposure The exception would include a young patient with an acute injury or repetitive extension activities, which can result in fracture of the pars interarticularis. Myelography (Myelogram) Largely replaced by MRI Generally not indicated in the evaluation of acute low back pain except in cases where the clinical picture supports a progressive neurologic deficit and the MRI and EMG are nondiagnostic. . Reserved as a preoperative test to correlate examination findings, often in conjunction with a CT scan. Discography (Discogram) Rarely necessary in the evaluation of acute low back pain and certainly not recommended within the first 3 months of treatment. Patients who have not responded to a wellcoordinated rehabilitation program or who have normal or equivocal MRI findings. May have some benefit in localizing a symptomatic disc as the etiology of nonradicular back pain. Computer Tomography (CT) Provides superior anatomic imaging of the osseous (bony) structures and good resolution for disc herniation. Its sensitivity for detecting disc herniation when used without myelography however is inferior to MRI. Magnetic Resonance Imaging (MRI) Should not be overused Has excellent sensitivity in the diagnosis of lumbar disc herniation and is considered the imaging study of choice for root impingement. Its use should therefore be reserved for selected patients. INDICATIONS OF MRI (IMMEDIATE) Patients with progressive neurologic deficit Cauda equina syndrome Patients with a suggestive presentation and known history or high risk for malignancy or inflammatory disease. Determining exact levels of pathology in the candidate for a selective nerve root block when physical examination and electrodiagnostic findings are not definitive. TREATMENT OPTIONS NON OPERATIVE TREATMENT OPERATIVE TREATMENT TREATMENT OPTIONS NON OPERATIVE TREATMENT OPERATIVE TREATMENT NON OPERATIVE TREATMENT REST DRUGS EXERCISES PHYSICAL THERAPY MODALITIES INJECTIONS APPROPRIATE DIAGNOSTIC TOOLS NEEDED TREATMENT OPTIONS NON OPERATIVE TREATMENT OPERATIVE TREATMENT NON OPERATIVE TREATMENT REST DRUGS EXERCISES PHYSICAL THERAPY MODALITIES INJECTIONS REST DECONDITIONING SHOULD BE AVOIDED AT THE ONSET BY LIMITING BED REST AND IMMOBILIZATION(2-3DAYS) LYING IN THE MOST COMFORTABLE POSITION(NOT RESTRICTED TO SEMIFOWLER OR LATERAL POSITION) MOST PREFER CONTINUATION OF ORDINARY ACTIVITIES WITHIN THE LIMITS PERMITTED BY PAIN AS SOON AS POSSIBLE DRUGS ACETAMINOPHEN Nonsteroidal Anti-inflammatory Drugs (NSAIDs) Muscle Relaxants Opioid Analgesics Oral Steroids Colchicine Anti-Depressant Medications Nonsteroidal Antiinflammatory Drugs (NSAIDs) Are a reasonable first-line medication Theoretically offer additional antiinflammatory effects(most prominent during the first week after injury) By carefully prescribing therapeutic doses at regular intervals, the analgesic and antiinflammatory properties of these agents will be best realized by the patient Prolonged use of these medications(greater than 4 weeks) should be avoided Muscle Relaxants Muscle relaxants can be used as short-term adjunctive medications Benzodiazepines (except low dose diazepam) do not appear to be helpful or indicated in patients with acute low back pain Commonly experienced undesirable side effects include drowsiness and fatigue Prescribed prior to bedtime to take advantage of their sedating effects and reduce daytime sedation. Anti-Depressant Medications Generally not necessary in the treatment of acute low back pain Tricyclic antidepressants, and in particular amitriptyline, have been well studied and supported as useful analgesics in patients with pain of neurogenic origin They can be helpful as adjuncts for pain and sleep if used at bed time Doses should begin low and slowly increased to minimize side effects Exercise to Optimize Outcome in Low Back Pain Improvement in aerobic fitness can improve blood flow and oxygenation to all tissues including the muscles, bones and ligaments of the spine Aerobic exercise may also decrease the psychological impact of low back pain by improving mood,decreasing depression, and increasing pain tolerance Active exercise program that emphasizes restoration of normal lumbosacral motion, trunk strengthening, and instruction in proper Transcutaneous Electrical Nerve Stimulation (TENS) It is generally used in chronic pain conditions and not indicated in the initial management of acute low back pain Success rates range greatly due to many factors including electrode placement, chronicity of the problem, and previous treatments Documentation of greater than 50% reduction in pain with a treatment trial may Electrical Stimulation High voltage pulsed galvanic stimulation has been used in acute low back pain to reduce muscle spasm and soft tissue edema (swelling) Its Use should be limited to the initial stages of treatment, such as the first week after injury so that patients may quickly progress to more active treatment, which includes a restoration of range of motion and strengthening It may often be combined with ice or heat to Ultrasound It has been found to be helpful in improving the distensibility of connective tissue, which facilitates stretching It is not indicated in acute inflammatory conditions where it may serve to exacerbate the inflammatory response It is best use to improve limitations in segmental spinal range of motion Ultrasound(cont.) The use of ultrasound is contraindicated over a previous laminectomy or peripheral nerve secondary to alterations in membrane stability It should be discontinued as segmental motion is improved with the patient then moved into an active strengthening program and eventual transference to an independent home Superficial Heat Superficial heat can produce heating effects at a depth limited to 1-2cm It has been found to be helpful in diminishing pain and decreasing local muscle spasm should be used as an adjunct to facilitate an active exercise program It is most often used during the acute phases of treatment when the reduction of pain and inflammation are the primary goals Cryotherapy Ice packs or cryotherapy are generally more effective in terms of depth of penetration than other superficial thermal modalities This is helpful in reducing local metabolism, inflammation, and pain The analgesic effects of ice result from a decreased nerve conduction velocity along pain fibers and a reduction of the muscle spindle activity responsible for mediating local muscle tone. Cryotherapy(cont.) It is usually most effective in the acute phase of treatment It is applied over an area for 15-20 minutes, 3-4 times per day initially and then on an as needed basis Peripheral nerve injury and local frostbite secondary to prolonged cryotherapy has been previously described, emphasizing the need for