Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Human microbiota wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Social history of viruses wikipedia , lookup
Triclocarban wikipedia , lookup
Globalization and disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
History of virology wikipedia , lookup
Sarcocystis wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Henipavirus wikipedia , lookup
Urinary tract infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Marburg virus disease wikipedia , lookup
West Nile fever wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Infection control wikipedia , lookup
Hepatitis B wikipedia , lookup
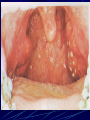
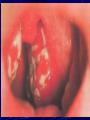
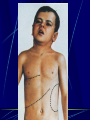
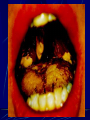
Diphtheria Tonsillitis is inflammation of the tonsils most commonly caused by a viral or bacterial infection. Symptoms of tonsillitis include sore throat and fever. Under normal circumstances, as viruses and bacteria enter the body through the nose and mouth, they are filtered in the tonsils. Within the tonsils, white blood cells of the immune system mount an attack that helps destroy the viruses or bacteria by producing inflammatory cytokines like Phospholipase A2, which also lead to fever. The infection may also be present in the throat and surrounding areas, causing inflammation of the pharynx. This is the area in the back of the throat that lies between the voice box and the tonsils. Primary tonsillitis The most common bacterial cause is Group A β-hemolytic streptococcus (GABHS), which causes strep throat. Less common bacterial causes include: Staphylococcus aureus (including methicillin resistant Staphylococcus aureus or MRSA ), Secondary tonsillitis (symptomatic) The most common causes of tonsillitis are adenovirus, rhinovirus, influenza, coronavirus, and respiratory syncytial virus. It can also be caused by EpsteinBarr virus, herpes simplex virus, cytomegalovirus. Specific tonsillitis Sometimes, tonsillitis is caused by an infection of spirochaeta and treponema, in this case called Vincent's angina or Plaut-Vincent angina. Sometimes – by fungi. Sometimes - by Corynebacterium diphtheriae Acute disease from the group of respiratory infections which characterized by fibrinous inflammation of mucous membranes of oral cavity, nasopharynx, larynx with toxic lesion of cardiovascular and nervous systems Etiology Corynebacterium diphtheriae Grampositive, nonmotile (Leffler rod) Don’t forms spores and capsules Coloured by Neisser in brown-yellow color Ru, Leffler, Clauberg mediums - blood agar with tellurium salts Cultural-biochemical types of C. diphtheriae - mitis, gravis, intermedius Production of very strong exotoxin (gene tox +) Structure of exotocin - dermanecrotoxin, hemolysin, neuraminidase, hyaluronidase Firm to low temperature, long save on a dry surfaces; high responsive to heating and desinfection solutions Epidemiology Source – sick person or carrier (convalescent or health) of toxicogenic strains Ways of transmission - airborne, contact household (occasionally) Sensibility is high, adults more often become sick (80 %) Case rate sporadic, outbreaks are possible Immunodefence antitoxic, postvaccine Seasonal character - autumn - winter Diphtheria cases reported to World Health Organization between 1997 and 2007 Pathogenesis Penetration of the agent through entrance gate (mucous of upper respiratory tract, sometimes conjunctivas, skin) Production of exotoxin Local and systemic effects of the toxin: Dermonecrotoxin - necrosis of a surface epithelium, retardation of blood stream, rising of a permeability of vessels, their fragility, transuding of plasma in ambient tissues, formation of a fibrinous film, edema of tissues; downstroke of pain sensitivity Pathogenesis Neuraminidase - replacement of cytochrome, blockage of cellular respiration, destruction of a cell, violation of a function of organs and tissues (central and peripheric nervous system, cardiovascular system, kidneys) Hyaluronidase - destruction of a stroma of a connecting tissue (rising of permeability of vessels, edema of tissues) Hemolysin - hemorrhagic set of symptoms Classification Localization - otopharynx, nose, larynx, trachea and bronchi; rare localizations (skin, eye) Degree of severity - mild, moderate, severy, hemorrhagic, hypertoxic Form - localized, wide-spread, combined Nature of process - catarrhal, island-like, paleaceous Complications - myocarditis, neuritis, nephritis (early and late) Subclinical (carriering) Clinical manifestation Incubation period – 2-10 days Phenomena of intoxication (high fever, malaise, general weakness, headache) Pharyngalgia - moderate Changes of a throat mucous - soft hyperemia, edema of tonsills, covers on their surface (grey colour, dense, hard to remove with bleeding, slime), spread out of tonsills limits (palatopharyngeal arches, uvula, soft palate) Augmentation and moderate morbidness of regional lymph nodes Edema of a hypodermic fat of a neck Peculiarities of diphtheria covers (Grey colour, dense, hard to remove with bleeding, slime), spread out of tonsills limits (on uvula, soft palate, palatopharyngeal archs) Edema of a hypodermic tissues of a neck Swollen neck in diphtheria Diphtheria of the nose A diphtheria skin lesion on the leg Features of diphtheria toxicosis (In wide-spread, combined, hypertoxical, hemorrhagic forms) toxicosis І, ІІ, ІІІ Edema of the neck hypodermic tissues Paleness of skin Cyanosis of lips Decreasing of arterial pressure Tachycardia Decreasing of a body temperature Diphtheria of larynx Real croup (stenosis of a larynx) І degree (catarrhal) - labored inspiration, retraction of intercostal spaces, rasping “dog barking" cough, “horse” voice ІІ degree (stenosis) - noisy respiration, inspiratory dyspnea with an elongated inspiration, participation in respiration of auxiliary muscles, aphonia ІІІ degree (asphyxia) - acute oxygen insufficiency, sleepiness, cyanosis, cold sweat, cramps, paradoxical sphygmus Complications Infectious-toxic shock Intra vessels disseminated syndrome Myocarditis (early, late) Polyradiculoneuritis (early, late) Nephrosonephritis etc. LABORATORY DIAGNOSTIC Detection of the agent in smears from a throat and nose (taking of material on border between effected area and normal mucous) Microscopy (colouring by Neisser) – typical locating of rods, grains of volutin in bacterias Sowing on convolute serum or telluric blood agar for allocation of clean culture and recognizing of toxigenisity Serological tests mirror a condition of immune defence (efficiency of vaccination) Treatment Immediate hospitalization Bed regimen (at localized forms - 10 days, at toxic not less than 35-45 days) Specific treatment - introducing of antitoxic antidiphtherial Serum (from 30-50 thousand IU at the localized forms up to 100-120 thousand IU at toxic, by Bezredka method) Glucocorticoids (in toxic forms and croup) Antibiotics (penicilini, tetracyclini, erythromycini) Strychninum (in toxic forms) In case of croup - inhalations, broncholitics, diuretics, glucocorticoids, antibiotics, antihistamine, lytic admixture; under the indications - intubation, tracheotomy Conditions of discharging from a hospital Clinical convalescence 2 negative results of bacteriological research of smears from a throat and a nose with two-day interval For decret group - additional double bacteriological examination in polyclinic Prophylaxis Plan immunization (vaccination in 3, 4, 5 months. With АPДT vaccine, revaccination in 18 months; 6, 11, 14, 18 years and adults every 10 years with АДT-М vaccine) In the focus – 7 days medical observation after contact persons Bacteriological examination Sanation of detected carriers Final disinfection Revaccination Desinfection Aeration and ultra-violet lighting of puttings, wet cleaning with usage of 2/3-basic salt of perchloron, calcium of hypochlorite, 3 % of solution of chloraminum, 1 % of solution amfolan Sputum, the outwashes from a nasopharynx hash with double quantity of solutions, exposition 2 hours. The tableware is boiled in 2 % potassium solution 30 mines. Bedclothes and clothes if necessary to decontaminate in desinfection camera Differential diagnosis Tonsillitis, including Plaut-Vincent-Simanovsky Herpetic tonsillitis ARVI (adenoviral infection, false croup) Paratonsillar abscess Infectious mononucleosis Scarlet fever Pseudotuberculosis Tonsillo-bubonic form of tularemia Mycotic affection of tonsills Epidemic parotitis Typhoid fever Lues Hematological diseases (acute leukosis, agranulocytosis) Common symptoms of tonsillitis sore throat red, swollen tonsils pain when swallowing high temperature (fever) coughing headache tiredness chills a general sense of feeling unwell white pus-filled spots on the tonsils swollen lymph nodes (glands) in the neck pain in the ears or neck changes to the voice or loss of voice The diagnosis of GABHS tonsillitis can be confirmed by culture. Samples are obtained by swabbing both tonsillar surfaces and the posterior pharyngeal wall are plated on sheep blood agar medium. The isolation rate can be increased by incubating the cultures under anaerobic conditions and using selective media. A single throat culture has a sensitivity of 90 %-95 % for the detection of GABHS. False-negative results are possible if the patient received antibiotics. The identification of GABHS requires 24 to 48 hours. Rapid methods for GABHS detection (10–60 minutes), are available. Rapid detection kits have a sensitivity of 85 to 90. Treatments to reduce the discomfort from tonsillitis symptoms include: pain relief, anti-inflammatory, fever reducing medications (acetaminophen/paracetamol and/or ibuprofen) sore throat relief (warm salt water gargle, lozenges, and iced/cold liquids) If the tonsillitis is caused by group A streptococus, then antibiotics are useful with penicillin or amoxicillin being first line. Cephalosporins and macrolides are considered good alternatives to penicillin in the acute setting. A macrolide such as erythromycin is used for people allergic to penicillin. Individuals who fail penicillin therapy may respond to treatment effective against beta-lactamase producing bacteria such as clindamycin or amoxicillin-clavulanate. Aerobic and anaerobic beta lactamase producing bacteria that reside in the tonsillar tissues can "shield" group A streptococcus from penicillins. When tonsillitis is caused by a virus, the length of illness depends on which virus is involved. Usually, a complete recovery is made within one week; however, symptoms may last for up to two weeks. Chronic cases may be treated with tonsillectomy (surgical removal of tonsils) as a choice for treatment. Complications Complications may rarely include dehydration and kidney failure due to difficulty swallowing, blocked airways due to inflammation, and pharyngitis due to the spread of infection. An abscess may develop lateral to the tonsil during an infection, typically several days after the onset of tonsillitis. This is termed a peritonsillar abscess (or quinsy). Rarely, the infection may spread beyond the tonsil resulting in inflammation and infection of the internal jugular vein giving rise to a spreading septicaemia infection (Lemierre's syndrome). In chronic/recurrent cases (generally defined as seven episodes of tonsillitis in the preceding year, five episodes in each of the preceding two years or three episodes in each of the preceding three years), or in acute cases where the palatine tonsils become so swollen that swallowing is impaired, a tonsillectomy can be performed to remove the tonsils. Patients whose tonsils have been removed are still protected from infection by the rest of their immune system. In very rare cases of strep throat, diseases like rheumatic fever or glomerulonephritis can occur. These complications are extremely rare in developed nations but remain a significant problem in poorer nations. Tonsillitis associated with strep throat, if untreated, is hypothesized to lead to pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS).[ Thanks for your Attention!