Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
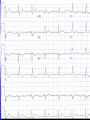
Interesting Case 82 year old man • Brought in to RAZ by EMS Presenting Complaint (nursing notes) “Ground level fall at 13:15 today. Unresponsive for 3 minutes after fall. No seizure, but incontinent of urine. Witnessed by wife.” What do you want to know? • BP 121/71 • HR 76 • RR 18 • O2 95% on 2 liters • T 36.7 Patient awake Confused Not oriented to place or time Doesn’t remember what happened Fortunately… • His wife is there Unfortunately… • She’s almost as confused as he is • She can tell you what happened, though History • Shopping – fell backwards while walking. • No prodrome • Hit back of head on floor Past Medical History • Two recent falls in the past month – wasn’t seen in hospital for these • Dementia • Rarely sees a doctor • No medications On exam • T 36.7 HR 76 RR 18 BP 121/71 O2 95% on 2 liters • CN exam normal • Hematoma right occiput • HR regular, no murmur • Wife thinks slightly more confused than usual •What next? •Any concerns? •Differential Dx? • Time to move • Needs a monitored bed • Investigations? Investigations • CBC, Lytes, Creatinine, Glucose, Mg, Phosphate, Calcium, Troponin • ECG • CT head and C-spine ECG • RBBB • Left Anterior Fascicular Block CT • CT C-spine normal • Cleared C-spine precautions CT head CT Head Report • Intraparenchymal hemorrhage involving bilateral posterior parietal lobes at occipital junction • Small SAH right frontal lobe • No midline shift Meanwhile… • Patient ticking along happily until… I hear some commotion… • Patient is slumped over and the monitor shows this rhythm • Asystole! •! •! •! • Spontaneous Resolution • Get the crash cart • Pads put on Quickly now… • Let’s have a talk about Level of Care • Full bore ahead Who ya gonna call? • A. Ghostbusters • B. Your Mom • C. The laundromat (underwear feels sort of damp) • Cardiology Next step • Transvenous Pacer • Patient agitated – required some sedation, but procedure otherwise successful Syncope • “Sudden transient loss of consciousness associated with inability to maintain postural tone.” Syncope • 1-3% of all ED visits • 1-6% Admissions Causes • Vasovagal, Carotid sinus syndrome • Neurologic – SAH, Subclavian steal • Medications • Orthostatic hypotension • Pulmonary Embolus • Cardiac Cardiac Syncope • 1. Structural – Aortic Stenosis, Cardiomyopathy, MI • 2. Dysrhythmias – Brady and Tachy Bradysrhythmias • 2nd or 3rd degree heart block • Sinus node disease • Pacemaker malfunction Tachydysrhythmias Ventricular tachycardia SVT A Fib A Flutter San Francisco Syncope Rules • CHESS • C – History of CHF • H – Hematocrit < 30% • E – Abnormal ECG • S – Shortness of Breath • S – Systolic Blood Pressure < 90 “Abnormal ECG” • Dysrhythmias • WPW • Brugada • Prolonged QTc • Any new abnormality Boston Syncope Rules • Broad set of rules – 25 criteria • Misses our patient Short-Term Prognosis of Syncope (STePS) • 4 Independent predictors – • 1. Abnormal ECG • 2. Concomitant trauma • 3. Absence of prodrome • 4. Male gender Back to our patient • Admitted to Cardiology • Transferred to Foothills for permanent pacer • Slow to recover from anaesthesia and transferred to ICU • Tachyarrhythmias – started on a metoprolol • Stabilized somewhat – transferred to CCU at PLC • Diagnosis of Sick Sinus Syndrome • No interventions regarding the intraparenchymal bleeds One more thing • Anchoring • Start with an anchor – something you know – and adjust in the direction you think is appropriate • Often not enough adjusting