Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
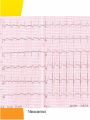
Emergency Department Management of Syncope Emilia McGhee Sept 2010 Syn.co.pe A transient loss of consciousness and inability to maintain postural tone due to global cerebral hypoperfusion. Characterised by a rapid onset, short duration and spontaneous complete recovery Incidence • • • • 1-3 % Emergency Dept visits 6 % of hospital admissions USA, Japan and Europe Occurs in up to 50% during lifetime (only 5% after 40 yrs) • Recurs in 30% • Due to cerebral hypoperfusion causing lack of oxygen and glucose supplly to brain • Cerebral perfusion maintained by: – Cardiac output – Systemic vascular resistance – Mean arterial pressure – Intravascular volume – Cerebrovascular resistance with intrinsic autoregulation – Metabolic regulation What is not syncope Transient LoC without global cerebral hypoperfusion • • • • Seizure TIA Metabolic disorders Intoxication Loss of postural tone without LoC • • • • • Cataplexy Drop attacks Falls TIA of carotid origin Functional psychogenic Syncope vs • Triggering factor • Prodrome • Convulsion after LoC, and <15 secs • Short duration • Quick recovery • Ongoing lethargy but no confusion Seizure • • • • • • • Pt history Aura Automatisms Convulsions at onset of LoC Longer duration Post-ictal phase Tongue biting, incontinence Classification • Reflex – neurally mediated – 30% • Orthostatic hypotension – 10-15 % • Cardiac – electrical and mechanical – 10% Reflex • Vasovagal – Emotional stress – Orthostatic stress • Situational – Coughing, micturition – GI stimulation – Post exercise, post prandial • Carotid sinus syncope – Uncommon, caused by pressure on carotid sinus – Head turning, tight collars shaving Orthostatic Hypotension • Primary autonomic failure – Pure auntonomic failure, multisystem atrophy, Parkinson’s Disease, Lewy body dementia • Secondary autonomic failure – Diabetes, amyloidosis, uraemia, spinal cord injuries • Drug induced – Alcohol, vasodilators, diuretics, phenothiazines, antidepressants • Volume depletion – Vommitting, diarrhoea, dehydration, haemorrhage “Syncope and sudden death are the same, except that in one you wake up” Cardiac - Electrical • Ventricular arrhythmias – VT, Torsades – Sudden onset, little prodrome – Elderly pts with known cardiac disease • Supraventricular arrhythmias – – – – SVT, AF with fast ventricular response Assoc with palpitations, chest pain, dyspnoea May occur on attempting to stand or walk Look for evidence of WPW, Brugada, Long QT • Bradyarrhythmias – Sick sinus, sinus brady, high grade AV block, adverse medication reactions, pacemaker malfunction – Chest pain, dyspnoea, decreased ET, fatigue Cardiac - Mechanical • Low CO output states – Cardiomyopathy, CCF, valvular insufficiency • Cardiac outflow obstruction – Sudden onset, no prodrome – Exertional in nature, murmur present – Aortic stenosis, HOCM, Mitral stenosis, pulmonary stenosis, pulmonary embolism, Lt atrial myxoma HOCM • Causes of syncope: – Self terminating ventricular arrhythmias – SVT – Severe outflow tract obstruction – Bradyarrhythmia – Hypotension in response to exercise – Reflex syncope Emergency Department Assessment • 45% can be diagnosed on history and exam alone • A cause will not be found for around 37% • Management is moving away from firm diagnosis to risk stratification of patients Aim in ED 1) Recognise life threatening conditions 2) Recognise low risk conditions for discharge 3) Chose appropriate FU for those who need further diagnostic testing 4) Recognise those who do not need further investigation History – High Yield Questions • What were they doing - at rest (arrhythmia) - exercise / post-exercise (AS, HOCM) - laughing, micturition etc • Was there a prodrome? - vasovagal • Did they have palpitations? - an arrhythmia • Were they SOB? - PE - tamponade • Did they have chest pain? - PE - ACS and an arrhythmia - dissection • Did they have abdominal pain? - AAA - ectopic • Did they have a headache? - SAH • • • • • Previous arrythmias Known CAD Sudden or unexplained deaths in family Known CCF Medications - QT prolonging medications - vasodilators - anti-hypertnesives Red Flags • • • • • Syncope during exertion Syncope in lying position Absence of external factors Family hx of SCD Slow recovery from syncope Examination and bedside tests • • • • • Cardiorespiratory exam Abdominal exam Neurological exam BSL Orthostatic BP – A drop of 20mmHg systolic, 10mmHG diastolic or increase in HR >20 – Systolic BP <90mmHg – Meaningful if they become symptomatic Ix that are helpful • ECG Consider on case to case basis: • FBC, EUC • Troponin, D.dimer, bHCG • UA • CXR • Echo • CSM • Tilt table • EPS • EST Ix that are generally low yield • • • • • CTB MRI Holter monitor Carotid dopplers EEG Important ECG findings • Evidence of AV conduction disorder – Prolonged PR – Mobitz 1 or 2 – CHB – RBBB or LBBB • Evidence of underlying cardiac disease – Rt or Lt axis deviation – Significant ST or T wave changes – Rt or Lt ventricular hypertrophy ECG findings associated with high risk of sudden cardiac death • • • • • • Hypertrophic cardiomyopathy Long QT Ventricular pre-excitation (WPW) Brugada Syndrome Short QT Arrhythmogenic Rt ventricular dysplasia ECG changes in HOCM • • • • • Normal in up to 15% Left axis deviation LVH and strain flipped T’s big voltage R waves and deep, narrow Q’s in lateral leads (I, aVL, V5 and V6) - infarct Q’s are > 1 small square where as HOCM Q’s are less than 1 small square Risk Scores • Risk scores should be applied once other identifiable causes have been considered • Do not replace clinical judgment and using your brain • Risk scores may miss rare causes with most serious outcomes San Francisco Syncope Rule C H E S S Congestive Cardiac Failure Haematocrit <30% ECG abnormal Shortness of breath SBP <90 at triage Any one of these factors predicts high risk and therefore pt should be admitted and investigated further SFSR • Endpoint was ‘serious outcome’ or any condition causing return to the hospital and admission • Sensitivity 96% and Specificity 56% for serious outcome at 7 days • Revalidated by external study in Canadian ED finding sensitivity 90%, Specificity 33% • Other studies found Sensitivity 52-77% • Blanket application to all syncopes and not just those with no diagnosis after ED evaluation ROSE Criteria • Predictors of serious outcome at 30 days – Raised BNP – Positive stool haemoccult – Anaemia – Hypoxia – Prescence of Q waves on ECG Sensitivity 87%. Negative predictive value 95.5% ACEP Recommendations Level A Level B Hx and exam suggesting CCF consistent with high risk Elderly, structural heart disease and coronary artery disease high risk Perform ECG Level C Echo, CT and other lab tests should not be routinely performed in absence of specific findings Admit CCF and structural heart disease. Other high risk: ECG abnormalities, haematocrit <30 What the studies agree on • Identified risk factors: – Age >65yrs – Hx of CCF – Abnormal ECG Normal ECG may include sinus tachy, first degree HB, non-specific ST/T wave changes. Syncope in the Elderly Most common causes • Orthostatic hypotension – 25% ‘Age related’ – 75% Medication related • Reflex – CCS cause in 20% • Cardiac arrhythmias – Advanced age, underlying cardiac disease and comorbidities Prolonged QT syndrome Brugada Syndrome WPW syndrome HOCM ECG changes in HOCM • • • • • Normal in up to 15% Left axis deviation LVH and strain flipped T’s big voltage R waves and deep, narrow Q’s in lateral leads (I, aVL, V5 and V6) - infarct Q’s are > 1 small square where as HOCM Q’s are less than 1 small square Epsilon waves in arrhythmogenic right ventricular cardiomyopathy Bifascicular block Trifascicular block ECG CHB ECG Tachy-bradycardia syndrome ECG Torsades des pointes Disposition of patients • Manage indentified cause as appropriate • Admit high risk for monitoring and investigation • Consider withdrawing medication likely to be responsible • Advise pts on how to avoid further syncope: – VVS – avoid stimulus – OH – medication change, good hydration, standing slowly – CSS – avoidance of tight collars, pressure on CS Future plans for Emergency Assessment – Recommendations from Europe • Falls and syncope service – Run by geriatrics, cardiology, neurology • Direct access to investigation and clinic – Tilt tables, Echo • Syncope observation unit – As part of MAU – 6 hr telemetry, hourly orthostatic BPs – Echo Assessing fitness to drive – National Transport Commission, Australia • Unexplained syncope: Private drivers refrain from driving for 3 months. Commercial for 6 months. • Recurrent syncope not responsive to treatment: criteria for conditional license not met • Cause of syncope identified and assessed as temporary – NO effect on driving status In the first 2 instances it is the responsibility of the patient to inform the RTA Driving fitness - Research • ESC: Data suggests that risk of a accident in pts with syncope is not different to those without • Prospective study of 3877 pts with syncope. Recurrence whilst driving occurred only in 10 pts. Risk of syncope related driving accidents is 0.8% per year. Summary • A syndrome encompassing many physiological and pathological processes • Our role is to identify those at risk of sudden cardiac death • Benign syncope, while having minimal mortality, has associated morbidity • Remember – Cardiac BAD, Non-cardiac Not so bad Thank You