Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
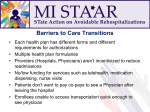
Reducing Readmissions by Engaging Patients and Families Kim McCoy, Stratis Health Teri Beyer, Rice Memorial Hospital September 11, 2012 RARE Campaign: Maintaining patient health after a hospital stay… …So We All Sleep More Peacefully. The RARE Campaign • A campaign across the continuum of care to reduce avoidable hospital readmissions across Minnesota • Focused on hospitals with support of providers, health plans, other key stakeholders • Designed to improve coordination of care and reduce fragmentation of the health care system Statewide Triple Aim Goals • Population health Reduce overall readmissions rate by 20% from 2009 baseline by December 30, 2012 • Care experience Enable patients to spend 16,000 more nights in their own beds instead of in the hospital • Affordability of care Save an estimated $30 million for commercially insured patients; additional savings for Medicare patients RARE Campaign Implementation Overview 2011-2012 Broad Community Support • Operating Partners • Institute for Clinical Systems Improvement (ICSI) • Minnesota Hospital Association (MHA) • Stratis Health (MN QIO) • Supporting Partners • Community Partners Geographic Representation Support for Hospitals • • • • • • RARE Resource Consultant Learning collaborative options Best practice toolkits Face-to-face sessions Webinars and conference calls Data reporting Five Key Areas • • • • • Comprehensive discharge planning Medication management Transition care support Transition communications Patient and family engagement Recommended Actions Report - http://rarereadmissions.org/documents/RARE_Recommended_Actions_Care_Transitions.pdf Patient and Family Engagement • Typical Transition Failures • Best Practices/Improvement Strategies • Proposed Measures • Gap Analysis • Tools and Resources Patient and Family Engagement • Use teach back to assess patient’s understanding of any instructions • Ensure caregivers are engaged in developing the plan of care • Use health literacy standards RARE Results to Date • 81 hospitals • 75 Community Partners across the care continuum • 2,607 readmissions prevented (13% reduction) • 10,000 more nights of sleep in their own beds http://www.rarereadmissions.org/ For more information… Kim McCoy, MPH, MS Program Manager Stratis Health [email protected] 952-853-8563 Rice – Reducing Readmissions Rice Memorial Hospital • City Owned Hospital • 100 bed Hospital (average daily census 60) • West Central MN – Willmar, MN (pop 20,000) • Service area 14 counties Key Players • • • • Rice Memorial Hospital Family Practice Medical Center Affiliated Community Medical Center Willmar Area Skilled Nursing Facilities – Rice Care Center – Bethesda Pleasantview & Bethesda Heritage – Willmar Care Center Hospital Team • • • • • • • • • • Administration Care Manager & Adult Health Care Director Discharge Planner/Social Work Care Manager Adult Health Care Nurse Respiratory Therapy Pharmacy Hospitalist Clinical Information Systems Finance Focus Areas • After Hospital Care Plan – Medication Management – Patient & Family Discharge Preparation • Discharge Advocate – Comprehensive Discharge Plan – Essential Transition Communication Elements • Follow –Up Support – After Discharge Follow Up – Community Partnerships After Hospital Care Medication Management - Home Medication List Accuracy • Trial of Pharmacist involvement in verifying the accuracy of the Home Medication List within 24 hours of Admission – Clinical Pharmacist completed an Admission Medication Review on 42 Family Practice Medical Center Patients – Interviewed Patient & Family as to what they were “actually taking” – Verified with Local Pharmacies – Checked Clinic List Medication List Accuracy – Pharmacy Review FINDINGS 66% had at least one discrepancy 50% had 2+ discrepancies Average of 1.9 per patient After Hospital Care Patient & Family Discharge Preparation • Patient & Family Learning • Daily Weights Patient & Family Learning - Healthcare Literacy • • • • 14% of all adults in the USA function below or at the 3rd grade level, 29% at a 6th grade level, 44% at 8-10th grade level, 13% > 10th grade level Patients who are older, racial/ethnic minorities, non native English speakers, low income levels and compromised health status have lower Literacy rates. Those with lower literacy rates have 4 times the healthcare costs than those with higher literacy skills. Patient adherence to Discharge Instructions affects hospital readmission rates. If patients do not understand the implications of their diagnosis and the importance of prevention and treatment plans, there is the potential for errors, adverse events, or unnecessary re-hospitalizations. WHAT and HOW we teach becomes even more important! Patient & Family Learning - Focus • • • • • Reason for hospitalization Tests, treatments & interventions New medications When to contact healthcare providers Follow-up appointments Patient & Family Learning “Teach Back” • Screen Pt/Family for Healthcare Literacy Level and Readiness to Learn • A scheduled time is arranged with patient and family • A Patient Teaching Method where the “learner teaches the teacher back” what they just learned. – Creates greater retention and recall – Allows for verification of learning Patient & Family Learning - Discharge Folders Pt/Family Discharge Preparation - Daily Weights • Daily weights to monitor for increasing weight while hospitalized – Often a sign of fluid overload – Can happens with IV Hydration, Medication Infusions or Blood Infusions – A reason for readmission – accumulation of fluid in the body in the lungs, lower extremities makes the work of the heart and breathing harder. Discharge Advocacy • Comprehensive Discharge Plan • Essential Transition Communication Elements Comprehensive Discharge Plan • Starts on Admission for Every Patient – High Risk Care Management Screening • Lives alone, over age 80, chemical dependency, frequent ESD or hospital readmissions, mental health concerns, inadequate support at home for care needs, receiving other services at home……. • Focused Discharge Planning and Care Coordination based on patient and caregiver needs to create a Safe Discharge Plan • Discharge Advocate Roles – Staff Nurse, Social Worker & Care Manager Essential Communication Elements - Discharge Summary Availability • Created a system to provide Primary Care Providers at the clinic with the Discharge Summary for the patient follow up visit – Hospitalists created a template to “tell the story” of the hospitalization including key components essential for follow-up care. – Faxed to clinics and scanned into clinic EMR’s Essential Communication Elements – Skilled Nursing Facilities • Participated in the Minnesota Hospital Association “Safe Transitions Pilot Project” • Included the Essential Elements of Communication in “Interagency Transfer Form” – Pressure Ulcer/Risk, Precautions, Pending Labs • “Hard Stop” Discharge Nurse to Admission Nurse Report & Order Review Follow-Up Support • After Discharge Follow Up • Community Partnerships After Discharge Follow Up - Follow Up Visits • Ward Secretaries meet with patient/family when scheduling follow-up appointments for them prior to leaving hospital – Clinic Post Hospitalization within 5-7 days • Previously up to 3 weeks (21 days) – Post ESD Visit within 3 days • Previously up to 2 weeks (14 days) After Discharge Follow Up - Post Discharge Phone Call Hospital Care Managers •Call based on risk Clinic Nurse •Call all patients within 72 hrs post discharge Community Partnerships • Cultivating Community Partnerships are Vital! • It takes a community focus and accountability to create the safety net for our patients. Readmissions/Safe Transitions In Care – MHA Statewide Goal – 20% less potentially avoidable readmissions from baseline in 2009 (Actual Rate/Expected Rate Ratio of 0.80) RMH Potentially Avoidable Readmission – RMH: • • • • 2009 Rate = 0.96 2010 Rate = 0.87 2011 Rate = 0.77 2012 Rate = 0.49 (1st Qtr data) Actual/Expected Rate Ratio 0.96 0.8 0.87 0.8 0.81 0.8 0.8 0.78 0.8 0.75 0.8 0.8 0.73 0.49 2009 2010 Q1 2011 Q2 2011 Q3 2011 RMH Actual/Expected Ratio Q4 2011 State Goal Q1 2012 Questions