Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
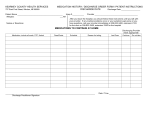
DISCHARGE SHEET Diagnosis:__ Date: _____________ Valuables: __ None Home meds: __ None Discharged: __ Walking Other with: __ Family to: __ Home Time: _______________ __ Returned to patient/family __ Returned to patient/family __ W/C __Stretcher __ Operation __ ________________________________________________ Wound ___ Site ______________ Condition _______________ Dressing __ Site ___________Condition____________ Condition: __ Good __ Stable __ Fair __ Poor V/S time: _____ T _____ P _____ R _____ BP ______ Elimination: __ Foley Date inserted ____ __ Voiding Foley size ____ __ Self __ Other ________ __ AMA __ Other ________ Instructions/Teaching Discharge Medications explained __ Take only those Diet explained: Written Material medications that have been approved by your Doctor. Provided __ Regular ___ Medication sheet provided: Yes No List meds taught: __ Soft ___ 1.___________________________ ___ ___ __ _______Calorie ADA ___ 2.___________________________ ___ ___ __ Clear Liquid ___ 3.___________________________ ___ ___ __ Other______________ ___ 4.___________________________ ___ ___ _____________________ 5.___________________________ ___ ___ 6.___________________________ ___ ___ 7.___________________________ ___ ___ 8.___________________________ ___ ___ Activity Level explained: Circle __ Resume normal daily activities __ Bed rest __ Up in chair __ Rehab services __ Other: _________________________ Explain: Prevention: Activities you can do to help decrease your chances of reoccurrence of acute episode: 1. 2. 3. List additional teaching material provided to patient/ Family: __ N/A __ Other______________________________ __ Pamphlet __ Booklet __ Video __ Instruction sheet List: I understand the instructions given. Signature of the Patient or responsible Party:_____________________ N:\Syllabus\Freshman\Spring\Discharge Summary Instructed by Dietician ___ ___ ___ ___ ___ Follow Up Appointment / Referrals: Keep all appointments __ Call Dr. Office and make an appointment on ____(date) __ To see Dr.________________________ on ____(date) Phone #_________________________________________ __ Referred to Agency: ____________________________ Phone #_________________________________________ Other: __ PT __ OT __ ___________________________ Phone #_________________________________________ Symptoms to watch for: 1. 2. 3. 4. What should you do: Special Instructions __ List: Discharge Nurse signature:_______________________ RN / LVN Reviewed 06/08