Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
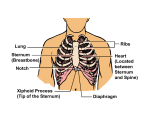
“Possibly, by focusing so much attention on discovering more effective drugs and more sophisticated defibrillator technology, we have lost sight of the vital importance of more mundane therapies, such as timely and proper provision of rescue breathing and chest compressions. Perhaps those who research cardiac arrest are guilty of the same oversight made by resuscitation team leaders – we have all been looking at the wrong aspects of the resuscitation attempt.” Stephen Pitts, Arthur L. Kellerman (Lancet 2004;364:314) The ResQ Trial: Comparison of Standard Cardiopulmonary Resuscitation (S-CPR) Alone vs. Active Compression Decompression CPR (ACD-CPR) Plus an Inspiratory Impedance Threshold Device (ITD) (ACD-CPR+ITD) on Survival from Out-of-Hospital Cardiac Arrest Learning Objectives After completing this course you will be able to: 1. Briefly describe the study objectives and your role in the ResQ Trial. 2. List the patient inclusion/exclusion criteria. 3. State the purpose of the randomization calendar and the method your agency uses to insure the calendar is followed correctly each week. 4. Describe the correct performance of standard CPR (with the modified hand position) and use of the AED according to current AHA guidelines. 5. Describe the correct performance of active compression-decompression (ACD-CPR) with the ResQ Pump and ResQ POD. Agenda • Study presentation • Manikin practice • Skills evaluation – Standard CPR with modified hand position – Use of an impedance threshold device (ResQ POD) – Performance of active compression decompression CPR with the ResQ Pump • Written evaluation – 80% correct (at least 12/15 questions correct) Funding Support Funding for this study is being provided by the National Institute of Health (NIH) grant #2-R44-HL065851-03 to Advanced Circulatory Systems, Inc. (ACSI), Eden Prairie, MN; Keith G. Lurie, MD, Principal Investigator. The contents of this presentation are solely the responsibility of ACSI and do not necessarily represent the official views of the NIH National Heart, Lung and Blood Institute. Study Purpose Evaluate the ability of two investigational devices to make Standard CPR (S-CPR) more effective: Active Compression Decompression CPR (ACD-CPR) – Performed with a ResQPump® Impedance Threshold Device (ITD) – ResQPOD® Why Does CPR Work? “Cardiac Pump” Theory Blood flow during CPR is due to the direct compression of the heart between the sternum and the spine. May play particularly important mechanistic role in early phases of CPR (valves lose competence after prolonged CPR). “Thoracic Pump” Theory • Ribs & sternum act as a bellows. • During chest compression, increased intrathoracic pressure, aided by one-way valves in the heart and venous system, cause forward movement of blood through the circulatory system. Decompression Phase • Blood returns to the heart during the relaxation (decompression) phase of CPR. • A small, but important, vacuum (negative pressure) forms in the chest relative to atmospheric pressure and draws blood back into the chest and heart. • The more blood that returns to the heart (preload), the more that is circulated forward (cardiac output) on the next compression. CPR with Incomplete Chest Relaxation 0 mmHg The desired negative pressure within this patient’s chest is never achieved. “Allowing complete chest recoil after each compression allows blood to return to the heart to refill the heart. If the chest is not allowed to recoil/re-expand, there will be less venous return to the heart, and filling of the heart is reduced. As a result, cardiac output produced by subsequent chest compressions will be reduced.” Highlights of the 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Currents in Emergency Cardiovascular Care. Vol. 16 No. 4, Winter, 2005-2006 Device Mechanisms • Goal: Enhance the negative pressure (or vacuum) in the chest during the decompression phase of CPR in order to return more blood to the heart. • ResQPump: Begins the creation of the vacuum • ResQPOD: Sustains the vacuum that is created Study Design • • • • • Prospective (using only “new” data) Randomized Multi-center (Whatcom Co. is 1 of 6 sites) Waiver of Informed Consent Sponsored by Advanced Circulatory Systems, Inc. (Eden Prairie, MN) • Funding support: NIH • Timeline: approximately 3 years to complete Study Sites MN: City of St. Paul (R. J. Frascone, MD) – MN: City of Minneapolis (Brian Mahoney, MD) – Minneapolis FD & Hennepin Co. EMS WA: Whatcom Co. EMS (Marv Wayne, MD) – Including Bellingham FD MI: Oakland & Macomb Co. (Bob Swor, MD) WI: City of Oshkosh (Tom Aufderheide, MD) - St. Paul FD Oshkosh FD MI: Ann Arbor (Bob Domeier, MD) Waiver of Informed Consent • Permitted by federal regs: 21 § CFR 50.24 • Qualifications – – – – – Life-threatening situation Obtaining informed consent is not feasible Prospect of direct benefit Research could not be done without a waiver Additional protections (next slide) Waiver of Informed Consent • Additional Protections – Community Consultation – Public Disclosure – Data and Safety Monitoring Board (DSMB) – Subsequent Notification – Written Informed Consent for continued participation Community Consultation • Open public meeting – Date/Time: June 30, 2005, 7-9PM – Location: Health Education Center • Surrogate community from which research subjects will be drawn – Variety of organizations & stakeholders • No veto power Public Disclosure • Communities in which study will be conducted; e.g.: – – – – Newspaper announcement Radio/TV spots Community organization newsletter Website • Plan for the investigation • Risks and expected benefits • Contact information Data and Safety Monitoring Board (DSMB) • Independent • Comprised of experts – e.g.: emergency medicine, neurology, bioethics, statistics, cardiology, anesthesiology • Responsible for oversight of safety – Monitor @ regular intervals • Authority to halt study CONFIDENTIALITY EMS personnel’s role is to maintain confidentiality of patient information at all times. Randomization • Definition: [n] The process of assigning study subjects to treatment (experimental) or control (standard of care) groups using an element of chance to determine the assignments in order to reduce bias. • Extremely important to follow when conducting research – Intention to treat Intention to Treat • Patients will be analyzed in the group that they should have received, not what they actually got. • Extremely important – Follow the schedule exactly – Implement the devices ASAP – Report errors Study Randomization • 2 arms – #1: CONTROL: Standard CPR (S-CPR) – #2: EXPERIMENTAL: ACD-CPR + ITD • Weekly randomization – equal, but randomly applied – week will begin on Sundays at 8AM – schedule is computer-generated and known in advance List at least two locations where you can find a copy of the calendar in your agency? Getting the Word Out Things we’re going to do in our system to make sure everyone knows what method of CPR they’re supposed to be performing: 1. Device availability (in color-coded bags) 2. Color-coded ResQ Trial calendar posted 3. Resource Guide in each vehicle (“rig folder”) Study Protocol (3100 pts) Cardiac Arrest Randomize by week S-CPR ACD-CPR + ITD Standard Treatment • Intubation • Defibrillation • IV & medications Outcome BLS & ALS Care • Only difference will be CPR method • Important: Equally aggressive regardless of CPR method • ResQPOD can be applied to: – Facemask (FIRST!) – ET tube (most preferred airway) – Combitube • Length of resuscitation: minimum 30 minutes Exceptional CPR Quality • Follow correct compression rates: – S-CPR: 100/min – ACD-CPR: 80/min • Allow chest to completely recoil • Do not hyperventilate – Facemask: 30:2 compression to ventilation ratio – Advanced airway: 8-10/min • Provide each ventilation over 1 sec • Avoid interruptions of CPR longer than 10 s Example: Vent rate: 48/min Switch Chest pressure seldom becomes negative The DANGER of Hyperventilation • • • • • • Seven pigs V-fib for 6 min Comp: 100/min Vent: 30/min CPR for 6 min Shock(s) as nec Survival: 1/7 (14%) • • • • • • Seven pigs V-fib for 6 min Comp: 100/min Vent: 12/min CPR for 6 min Shock(s) as nec Survival: 6/7 (86%*) *P<0.05 Inclusion Criteria • Adults known or presumed to be ≥ 18 yrs • Presumed* non-traumatic cardiac arrest – – – – – – – – – Cardiac etiology Respiratory etiology Stroke Overdose Smoke inhalation Drowning Burns Metabolic imbalance Seizures *If you are uncertain, presume it is non-traumatic until you discover otherwise Exclusion Criteria • Known or presumed < 18 years • Obvious or likely traumatic etiology – Penetrating or blunt trauma • • • • Pre-existing DNR orders Obvious signs of clinical death Family members who request exclusion For ACD-CPR+ITD arm: recent sternotomy (wound not appearing completely healed or, if known, < 6 months) Study Endpoints • Primary: Survival to hospital discharge • Secondary: – Return of spontaneous circulation (pulse) – Survival to: 1-hour, 24 hours, ICU admission, 30 days, 90 days & 365 days – Neurologic recovery @ hospital discharge, and 30, 90 & 365 days – Adverse events & complications Study Scene Monitor • Research personnel will be making random scene responses to – Monitor quality of CPR – Make sure devices are being used properly – Act as a resource in the field Name at least one way to find the answers to your questions about adult CPR and the ResQ Trial. Run Follow-up • Complete patient care record accurately • Call in to research hotline (24/7) – 1-866-640-2832 – ALL ARRESTS; regardless of whether entered and regardless of resuscitation attempted • ResQPOD: place sticker on run report; dispose of ResQPOD unless there were problems; replace with new • Clean ResQPump and reuse; record device number on run report Benefits to Patients • Possibly an opportunity for improved survival (but this is not guaranteed and is unknown at this time) • Opportunity to contribute to the scientific knowledge base that may benefit others • Patients in the control group may benefit as well – Hawthorne effect Risks to Patient • Vomiting during CPR (EMS hotline report) • Chest fractures (verified by CXR) • Pulmonary edema (EMS hotline report: airway fills with fluid twice; and/or CXR) • Organ damage (chart review or autopsy) • Chest bruising or redness (EMS hotline report) • Death (EMS hotline report and chart review) • Survival with neurologic damage (chart review) • Device performance/failure (EMS hotline report) Hotline Report (example questions) • • • • • • • • • • • • • • Did you attempt resuscitation on the patient? If not, why? Was the patient believed to be at least 18 yrs old? If not, age: Was the likely cause of the arrest non-traumatic? Was the likely cause of the arrest presumed to be cardiac? Did the patient have preexisting DNR orders or did you stop efforts early because of the family’s request? Did family or bystanders request that the experimental devices not be used? Did the patient have a recent sternotomy? Was the patient a prisoner? Was the patient known or suspected to be pregnant? Did EMS perform 1-59 seconds of CPR on the patient? Did the patient have a complete airway obstruction that could not be cleared? Did you attempt to intubate the patient with an ET tube or Combitube? If yes, were you successful? Standard CPR (S-CPR) • Package with facemask only • Airway not secured (facemask) – Compression to ventilation ratio 30:2 – Compress to 1.5 - 2” & allow complete recoil with modified hand position – Compress at rate of 100/min but pause for breaths – Ventilate over 1 second • Airway secured (ET or Combi-tube) – Compress continuously @ 100/min; do not pause for breath – Compress to 1.5 – 2” & allow complete recoil with modified hand position – Ventilate at 8-10/min (1 breath about every 6-8 seconds) – Ventilate over 1 second Hand Positions for S-CPR Old New ResQPump™ Metronome Force Gauge Suction Cup Handle ACD-CPR Compression • Same as standard CPR • 1 ½ - 2” • Compression rate 80/min Body position is critical to avoid fatigue. Perform CPR at patient’s side. Rotate compressor role @ every 2 minutes. ACD-CPR Decompression Lift until force gauge reads approx. –20 to –30 lbs Most common error is failure to actively decompress chest ACD-CPR + ITD • ResQPump & package with facemask, ResQPOD & sticker • Place ResQPOD on facemask ASAP – Hold tight facemask seal at all times • Airway not secured (facemask) – Compression to ventilation ratio 30:2 – Compress to 1.5 - 2” with active decompression (use gauge) – Use ResQPump & compress @ 80/min (metronome); pause for breaths (less than 10 sec) – Ventilate over 1 second • Airway secured (ET 1st choice) – Compress continuously @ 80/min (metronome); do not pause for breaths – Compress to 1.5 – 2” with active decompression (use gauge) – Move ResQPOD to airway and turn on timing assist lights – Ventilate according to lights or 8-10 breaths/min – Ventilate over 1 second Hand placement to maintain a tight seal Two-person rescue breathing* One person rescue breathing *The two-handed technique is preferred. When it’s time to pause compressions to give the breaths, the person doing chest compressions can reach over and squeeze the ventilation bag. ResQPOD with an ET Tube The timing-assist lights should be turned on to guide ventilation rate (or 8-10 breaths/min.) only after an advanced airway is placed. (Disconnect the ResQPOD to deliver meds thru ET tube, then reconnect and continue ventilations.) The ResQ POD is a CPR Tool If CPR is in progress… When pulse returns… ETCO2 Monitoring Place the ETCO2 sensor between the ventilation source and the ResQPOD. Troubleshooting • Timing assist light function is independent of inspiratory impedance valve feature. • If timing assist lights fail to operate or appear to blink at a rate different than 10/minute, disregard the lights, continue using the ResQPOD, and ventilate the patient at 8-10 breaths/minute. • Discontinue ResQPOD if: – Chest does not rise with ventilation – Device appears to malfunction in any way – The POD fills with fluid twice (the airway may be suctioned as needed) Troubleshooting ResQPOD Fills With Fluid • Clear fluids or secretions from the ResQPOD by removing it from the airway adjunct and blowing out debris using the ventilation source. • Discontinue use if the device cannot be cleared. • Discontinue use if the ResQPOD fills with fluid more than once. – May replace POD with new one (preferred), or d/c completely – Suctioning of tube (w/o fluid in POD) does not require that the POD be discontinued • If any problems with the ResQPOD, save in a red bag and return to study coordinator Troubleshooting ACD-CPR • Suction problems in 10-15% of patients – – • May interfere with AP patch placement – • Check placement and continue Hickey or bruising to chest – • Rotate frequently Rib fractures – • Move patches Requires 25% more rescuer energy – • Reposition, shave, or dry off chest Continue use unless distracting Continue Discontinue use if device appears to malfunction. ResQ Pump Cleaning/Reuse • Clean cup with soap and water. • May be cleaned with bleach solution or other disinfectant. • Check gauge for proper calibration. Untrained Healthcare Providers Do not leave the ResQPOD or ResQPump in the hands of healthcare providers who have not been trained in their use.