Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
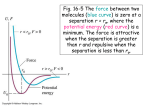
Safe Monitoring of Intramuscular Rapid Tranquilization - Audit Dr. Karolina Szumanska-Ryt, Dr. Ruth Collins, Dr. John Cooney St. Michael’s Unit, Mercy University Hospital, Grenville Place, Cork, Ireland Introduction Gold Standard Rapid tranquilisation (RT) is defined as the use of medication to calm/lightly sedate the service user, reduce the risk to self and/or others and achieve an optimal reduction in agitation and aggression. This should allow for a thorough psychiatric evaluation to take place with comprehension and response to spoken messages throughout the intervention. It is recognised that rapid tranquilisation may lead to deep sedation/anaesthesia, although this is not the overt intention. It is therefore important to ensure that vital signs are frequently monitored to avoid any possible adverse effects as a result of intramuscular RT. Based on a review of international guidelines, the following were developed as the gold standard of the audit; All physical restraints (100%) which required intramuscular rapid tranquilization had immediate and regular monitoring 5 - 10 minutes for the first hour 30 minutes for the next 2 hours Should a repeat intramuscular rapid tranquilization occur, the same monitoring standards were examined. Aim The purpose of this audit was to assess the current monitoring standards of vital signs and to identify any adverse events that may have resulted in relation to poor monitoring. Methods This is a retrospective audit examining the clinical practice forms for physical restraints between November 2006 and December 2009. Thorough examination of case notes present within ward filing system to identify the cases which required IM rapid tranquilization. Physical restraints which did not required IM rapid tranquilization were excluded in the audit. Inspection of commonly used tranquilizing agents and their effectiveness. To assess if any adverse events occurred. Results A total of 92 physical restraints were examined. Of these, 62 required IM RT. 12 RT were repeated events (24%) Fig. 1. The gold standard was not achieved as there was no evidence of safe monitoring (0%) Fig. 3. Adverse events were seen in 19% of overall cases, of these 40% were seen in repeat RT events. Most commonly used agents were a combination of benzodiazepine + antipsychotic (52%). Single agent use was associated with a higher risk of repeat physical restraint and RT (32%) versus combination of agents (18%) Fig. 4. Evidence of Safe Monitoring An adverse event was defined as; Gold Standard (100%) RT resulted in direct injury to patient as a result of poor monitoring of vitals and patient. High dose administering or unsafe combination use without monitoring of vitals. Clinical situation prior to RT is deemed unsafe and would warrant closer monitoring of vitals. Mean arterial pressure (MAP) < 70 based on documented vitals and no action taken. no Evidence of Safe Monitoring (0%) Evidence of Safe Monitoring Data was collected with standard pro forma and basic statistical calculations were used. 92 Physical Restraints examined -> (30 no IM Rapid Tranquilization) Fig. 3. Results of safe monitoring -> 62 IM Rapid Tranquilization 50 Initial IM Rapid Tranquilization 12 Repeat IM Rapid Tranquilization Medications RT (n= 50) Required a repeat RT (n= 12) Total repeat RT Benzodiazepine 12 (24%) 4 (33%) 7/22 single agent use (32%) Antipsychotic 10 (20%) 3 (30%) Benzodiazepine + Antipsychotic 26 (52%) 4 (15%) Antipsychotic + Antipsychotic 2 (4%) 1 (50%) (24%) Fig. 1. Breakdown of RT events RAPID TRANQUILIZATION RECORDING FORM: Name Consultant 5/28 combination agent use (18%) Date/Time MHA Status List the medication given during the episode of Rapid Tranquilization Medication Dose Time Route Fig. 4. Types of agents used in RT Notes Conclusions Please note, this is NOT a prescription Physical Monitoring: Alertness Respiratory rate Pulse Blood pressure Temperature Spo2 1. Every 5-10 minutes for 1 hour 2. Then every 30 minutes until patient is ambulatory 3. Then continue to monitor alertness, mental state and behaviour. Restart physical observations if there are any concerns. The use of a single agent (22 cases) was associated with a higher risk of repeat RT versus the use of 2 agents in combination (28 cases) Fig. 4. Fluid balance & electrolyte balance should be monitored as clinically indicated ECG monitoring is recommended when parenteral antipsychotics have been given in high doses If a patient is unconscious continuous pulse oximetry is recommended Time: Respiratory Rate / min Pulse / min 02 Saturations Blood Pressure Temp Alertness Adequate monitoring of vital signs could have prevented many of the adverse events seen in this audit. Evidence also suggests that training of staff in both monitoring of patient and the use of de-escalation techniques can prevent and provide safe RT to the service user. Signature (see chart below) Baseline: The following were recommendations from the results of the audit; A V P U Alert: Eyes open with normal verbal response. Voice: Eyes closed but will open eyes on command, and with normal verbal response. Pain: Eyes closed, responds to painful stimuli (nail bed depression – finger or toe nail). Unresponsive: Does not respond to ANY of the above. Completely unconscious Summary: (Main issues should be recorded in case notes including comments from service user or adverse events) Staff Name: Fig. 2. RT vital sign monitoring form Propose a document for vital sign monitoring (Fig. 2) along with guidance on managing common adverse events Incorporate this document into the development of a departmental guideline for IM rapid tranquilization Incorporate the IM RT guideline into the induction teaching program to raise awareness of key management decisions. Training for all staff members in; Preventative measures – recognizing risk situations De-escalation techniques Use of monitoring equipment Resuscitation skills and equipment training Re-audit to complete cycle