Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
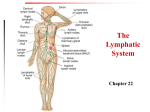
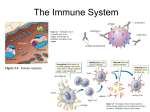
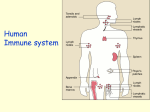
OBJECTIVES • Understand and define the terms allergic reaction and anaphylaxis explaining the difference between a local and systemic reaction. • Describe the five categories of stimuli that can cause an allergic reaction or anaphylaxis • Explain the importance of managing the Airway, Breathing and Circulation of a patient who is having an allergic reaction. • Outline the management steps for a patient with a local or mild allergic reaction • Outline the management steps for a patient with a severe systemic allergic reaction/anaphylaxis IMMUNE SYSTEM Two distinct, cooperative systems Natural/Innate Immune System is a generalized defense system against any foreign invaders. Everyone is born with a functioning Natural/Innate Immune System Learned/Acquired Immune System is gained through both passively and actively being exposed to a foreign pathogen. Everyone develops their own Learned/Acquired Immune system specific to that individual. INVADERS “IF YOU’RE NOT WITH US, YOU ARE AGAINST US!” • What types of things invade the body triggering the immune system? • Pathogens – disease producing agent: a virus or other microorganism • Antigens– foreign proteins that trigger the release of antibodies • Immunogens – a cell or substance that triggers immune response DEFENSE SYSTEMS Natural Immunity (Everyone has) Anatomical Barriers – Skin, mucous membranes Inflammation Acquired Immunity (Specific to the individual) Antibodies – bind with the receptor site of an antigen, disabling it and/or signaling of its existence to other parts of the defense system to be destroyed ANATOMICAL SURFACE BARRIERS • First Line of Defense in Immune Response Skin First line of defense against any foreign invader Mucus Membranes at natural openings Antibacterial Serve to protect internal systems with open links to the outside such as the respiratory and gastrointestinal systems PROTECTING INTERNAL SYSTEMS GI Tract Saliva Turbulence of swallowing Low pH of stomach Natural bacteria of gut Airway Mechanical ejection of pathogens through coughing Mucus membrane sloughing Urinary Tract Acidic Antibacterial mucosa Sphincters to inhibit backflow INFLAMMATION • Second Line of Defense in Immune Response General – Non specific to the type of invader All available foot soldiers called into action – Immune system is activated and immune cells respond to the effected site to begin removal of pathogens INFLAMMATION • Immune Cells (white blood cells) responding to site of invasion will take part in a variety of processes: Destroy and remove unwanted substances Dispose of invaders • Wall off infected/injured area Prevent spread of damage • Stimulate immune process Call up more White Blood Cells • Promote healing Set stage for repair TISSUE INJURY: WHAT HAPPENS THAT RESULTS IN INFLAMMATION? Causes release of chemical mediators Histamine – Kinins – Prostaglandins are examples Vasodilation of arterioles Increased blood flow to area of injury Increased heat due to increased blood flow Increased metabolic rate– use more glucose Permeability of capillaries Leak fluid into interstitial space between blood vessels and cells Shortens diffusion route of oxygen and glucose from blood vessels to cells Increased oxygen and nutrients to injured cells Increased edema due to extra fluid in interstitial space Pressure on pain neurons due to extra fluid in interstitial space FOUR CARDINAL SIGNS OF INFLAMMATION Redness Heat Swelling Pain HOWEVER IF IT GOES OVERBOARD . . Inflammation causes Bronchoconstriction Vasodilation Increased vascular permeability Increased gastric motility Can cause a medical emergency LEARNED/ ACQUIRED IMMUNE RESPONSE • • • • • • Third Line of Defense in Immune Response Elite Group of soldiers - Antibodies High tech weapons Specific targets Takes time to mobilize Depend on inflammation to begin battle ANTIBODIES • Made by specific white blood cells – B lymphocytes • B lymphocytes are specific to the individual person • B lymphocytes create antibodies after exposure to specific antigens to protect the body • B lymphocytes also create memory cells to recognize the antigen if it appears again and call up the antibodies ANTIBODIES ACT TO….. • Directly destroy or neutralize foreign antigen • Call up white blood cells to assist in destroying antigen • Indirectly call up increased inflammation response IF THE ANTIGEN APPEARS AGAIN. . . • Recognized by B memory cells • Located and identified by antibodies • White blood cells called in to destroy the antigen • The antibody response is stronger each time the antigen appears. INAPPROPRIATE IMMUNE RESPONSES Auto Immune Disorders: Body allergic to itself Arthritis Lupus Exaggerated Immune Response Hypersensitivity Allergic Reactions Anaphylaxis ALLERGENS: WHAT CAN CAUSE AN ALLERGIC REACTION? • Antibiotics • Foreign Proteins • Foods: eggs, shell fish, MSG • Insect Stings • Hormones • Blood Products • Preservatives • X-ray contrast media SIGNIFICANT ALLERGENS To cause an allergic reaction an allergen must be: • Significantly foreign • Significantly large • Significantly complex • Present in significant amounts ALLERGIES Hypersensitivity– Mild allergic reaction Delayed response to an antigen Results does not involve antibodies. Commonly results in skin rash. Results from exposure to certain drugs or chemicals. Allergic to soaps or detergents ALLERGIC REACTION VS ANAPHYLAXIS Allergic Reaction An exaggerated response by the immune system to a foreign substance/ antigen not always life threatening Involves antibodies Anaphylaxis An unusual or exaggerated allergic reaction to an antigen A life-threatening emergency ALLERGIC REACTION Rapid Response Inflammation Response Antibodies created • First response may be mild • Following responses will be more rapid and severe Generalized Reaction Mucus membranes swelling Skin --hives Respiratory Tract -- swelling Circulatory System---capillary leaking Gastrointestinal– vomiting and diarrhea ANAPHYLAXIS: SEVERE ALLERGIC REACTION Most anaphylaxis results from an injected antigen. Antigen rapidly distributed throughout the body, resulting in massive inflammation and antibody reactions. Most common Antibiotic injections Insect stings. Affects cardiovascular, respiratory, gastrointestinal systems and skin Significant fluid loss through increased capillary leaking ANAPHYLACTIC SHOCK • Caused by widespread vascular dilation increased capillary leaking bronchoconstriction • Can cause severe • respiratory distress • dizziness • fainting, coma • respiratory and cardiac arrest ANAPHYLACTIC SHOCK • Patient will have: hives, flushed skin edema (especially of the tongue, face, and lips) stridor from the upper airway, and wheezes altered LOC and cyanosis during later stages. signs and symptoms of shock hypotensive tachycardia May be deadly due to poor oxygenation and perfusion MANAGEMENT: STABLE MILD/MODERATE ALLERGIC REACTION V – Vital Signs O - Oxygen M – Cardiac Monitor (When available) I – Intravenous Access (When available) Fluid bolus to raise BP T – Treatment (medications) and Transport Consider the need for medications: Epinephrine: SubQ 1:1000 0.3- 0.5 ml Diphenhydramine (Benadryl) 25-50 mg IV/IM Nebulized Duoneb EPINEPHRINE • Used in cases of moderate allergic reactions and anaphylaxis • Administered via auto injector (0.3mg IM for adult or 0.15mg IM for peds) or by ALS providers 0.3mg SQ for adults and 0.01mg/kg for peds. **Note concentration is 1:1000 • Serves as a vasoconstrictor to raise blood pressure • Serves as a bronchodilator to relieve respiratory distress and stridor • Need to monitor vital signs after administration; pulse and blood pressure will be effected • Some patients may carry their own Epi-Pen to use in case of an allergic reaction DUONEB • Consists of 3mg Albuterol and 0.5mg Ipratropium in 3ml normal saline • Is used as a bronchodilator for patients who are experiencing wheezing and/or diminished lung sounds • Administered with oxygen via a nebulizer at 8-10 LPM • Requires reassessment of patient vital signs between Duoneb treatments • Can be given to patients in severe respiratory distress or respiratory arrest via a BVM with an inline nebulizer kit DIPHENHYDRAMINE (BENADRYL) • Used as an anti-histamine to block the naturally occurring effects of inflammation involved in the reaction • Given only by ILS/ALS providers • Dosages are 50mg IVP or IM for adults; 1mg/kg IVP or IM for peds • Monitor patient vital signs after administration USE COMMON SENSE • Do all patients get all treatments listed in protocol? • Does everyone with hives and itching need Epinephrine? Epinephrine is only administered to patients with respiratory difficulty and wheezing or signs and symptoms of shock • What if no wheezing? Does this patient require a Duoneb treatment? • History of cardiac disease? Will the Epinephrine have a negative effect on the patient 6 ‘RIGHTS’ OF MEDICATION USAGE Before giving any medications be sure you know: Right Medication Right Route Right Time Right Patient Right Dosage Right Documentation MANAGEMENT: SEVERE ALLERGIC REACTION UNSTABLE ANAPHYLAXIS V – Vital Signs O - Oxygen M – Cardiac Monitor (When available) I – Intravenous Access (When available) Fluid bolus to raise BP T – Treatment (medications) and Transport Needs medications!! Epinephrine: SubQ 1:1000 0.3- 0.5 ml Diphenhydramine (Benadryl) 25-50 mg IV/IM Nebulized Duoneb If patient experiences respiratory arrest or if respiratory arrest is imminent, ALS providers should contact Medical Control to administer Epinephrine 1:10,000 0.3-0.5 mg IV ONGOING MANAGEMENT • Reassess critical patients every 5 minutes • Reassess non-critical patients every 10 minutes • Monitor lung sounds, O2 saturation, respiratory rate, and heart rate • Reevaluate patients skin for signs of redness and hives CASE STUDY 1 Dispatch: 1800 to a residence for a 61 year old male patient with tightness in his chest and trouble breathing SCENE SIZE UP Scene Safety: Private home; no signs of potential danger, large porch with 4 steps to get onto porch; Taken to dining room where patient is seated; Note half eaten dinner roses and a strong odor of garlic BSI: Gloves Nature of Illness: Respiratory Distress Number of Patients: 1 Additional Resources: ALS Intercept (If Applicable) PRIMARY ASSESSMENT General Impression: The patient is sitting in an upright position at end of table Level of Consciousness: Awake, alert and obeys commands. Airway: Open, clear Breathing: Respirations fast and shallow; lungs clear Circulation Skin: pale, normal in temperature and dry Pulses: Radial pulse weak and rapid Bleeding: None Rapid Head to Toe: Note hives on chest and neck Priority: Stable FOCUSED HISTORY Signs and Symptoms: Began having trouble breathing while eating dinner Allergies: none known Medications: Nitro-patch, Lasix, and Zestril Past Medical History: Uncomplicated MI 2 years prior, Hypertension, and Congestive Heart Failure Last Oral Intake: Eating Shrimp Scampi when trouble breathing began Events: No complaints prior to eating; sudden onset DETAILED PHYSICAL EXAM Note hives on chest and neck Breathing short and shallow but lung sounds clear Vital signs: Blood Pressure: 118/70 Pulse: 128 Respiratory: 28 O2 Saturation: 91% Blood Sugar: 91 CRITICAL THINKING • Is this patient stable or unstable? • How aggressive do you need to be with him? • Does he need epinephrine? • What might happen to this patient if you gave him epinephrine considering his past history of heart disease? MANAGEMENT Interventions Oxygen to keep patient O2 Saturation above 94% Ongoing Assessment Patient voices relief with oxygen Repeat Vital Signs: Blood Pressure: 116/70 Pulse: 110 Respirations: 20 O2 saturation: 100% on Oxygen at 4lpm CASE STUDY 2 Dispatch: 1100 to a residence for a 38 year old male patient unresponsive SCENE SIZE UP Scene Safety: Private home; no signs of potential danger, easy access with patient laying in kitchen near side door BSI: Gloves Nature of Illness: Unresponsive Number of Patients: 1 Additional Resources: ALS Intercept (If Applicable) PRIMARY ASSESSMENT General Impression: Patient is prone in kitchen, does not move as you come into the room Level of Consciousness: Unresponsive to verbal or painful stimuli Airway: Open but stridor noted Breathing: Respirations are labored; poor rise and fall of chest; audible wheezes Circulation Skin: pale, cool, and cyanotic Pulses: No radial pulses with weak carotid pulse Bleeding: None Rapid Head to Toe: Large, blotchy hives over most of patients skin Priority: Acute status; initiate ALS Intercept immediately and correct ABCs FOCUSED HISTORY Signs and Symptoms: Was in garage when he found a bee hive; came into kitchen and collapsed in front of wife, who is able to assist with your assessment Allergies: Bee stings, but never had a reaction this bad Medications: Has an Epi-Pen but wife was unable to locate it Past Medical History: None Last Oral Intake: Breakfast 2 hours ago Events: No complaints prior to collapsing, but wife says it looked like he couldn’t breathe DETAILED PHYSICAL EXAM Hives over most of body Pupils reactive but sluggish No purposeful movement with GCS of 3 Vital signs: Blood Pressure: Unable to obtain via palpation or auscultation Pulse: 140 felt at carotid Respirations: 6 Oxygen Saturation: 68% Blood Sugar: 110 MANAGEMENT • Oxygen at 100% via Bag-Valve-Mask • Consider need for Spinal Motion Restriction • (ALS) Initiate Intravenous Access with 0.9NS at wide open rate • (ALS/BLS) Duoneb through Inline Nebulizer • (ALS/BLS) Administer Epinephrine as appropriate; ALS consider need to contact medical control for Epinephrine 1:10,000 IVP • (ALS) Benadryl 50mg IVP Ongoing Assessment After medication administration, patient is now awake and anxious; hoarse voice Repeat Vital Signs: Blood Pressure: 110/70 Pulse: 110 Respirations: 16 O2 saturation: 94% with Duoneb treatments and Oxygen at 100% through NRB REVIEW • If doing this CE individually, please e-mail your answers to: [email protected] • Use “June 2014 CE” in subject box. • IDPH site code: 06-7100-E-1214 • You will receive an e-mail confirmation. Print this confirmation for your records and document in your PREMSS CE record book. TRUE OR FALSE? 1. Every allergic reaction is considered to be anaphylactic 2. Every patient that has an allergic reaction should receive epinephrine 3. The skin is a natural barrier against antigens TRUE OR FALSE? 4. The common signs of inflammation are redness, heat, swelling, and pain 5. Lupus is an auto-immune disorder 6. Inflammation release causes vasoconstriction TRUE OR FALSE ? 7. Anaphylaxis is a serious medical condition that could result in the death of the patient 8. An allergic reaction is an exaggerated response by the immune system to a foreign substance TRUE OR FALSE? 9. The 6 ‘Rights’ of medication administration are: Right Patient, Right Time, Right Medication, Right Dosage, Right Route, Right Documentation 10. A patient does not need to be reassessed between administration of Duonebs TRUE OR FALSE? (ALS) 11.A Patient in respiratory arrest should be treated with Epinephrine 1:10,000 IVP AFTER contacting Medical Control 12.Benadryl is a histamine blocker 13.Epinephrine will have no effect on patient heart rate or blood pressure ANSWERS 1. False 2. False 3. True 4. True 5. True 6. False 7. True 8. True 9. True 10. False 11. True 12. True 13. False