Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hygiene hypothesis wikipedia , lookup
Epidemiology wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Public health genomics wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Marburg virus disease wikipedia , lookup
Infection control wikipedia , lookup
Fever of Unknown Origin in a
Tracheostomy- and VentilatorDependent Child
Kensho Iwanaga, MD
Fellow, Pediatric Pulmonology
03.23.11
History of Present Illness
• 4 y/o girl with tracheostomy and nighttime ventilator
dependence for BPD and UAO with acute respiratory
distress
• Nasal congestion and decreased activity x24 hours
• Fever to 103 °F overnight
• Unable to come off the ventilator this morning
• Low-grade fevers and greenish drainage from the
tracheostomy stoma site for the last 5 months
CRP (mg/dL)
WBC (k/mm3)
History of Present Illness
Ceftin/TOBI
(clinic)
Past Medical History
•
•
•
•
•
25-5/7 weeks gestational prematurity
Moderate-severe BPD
Tracheostomy for severe subglottic stenosis
Oral aversion with G-tube dependence
Baseline respiratory support
• Day: HME + 0.5 L/min oxygen
• Night: Ventilator + 1 L/min oxygen
• IMV 12, PIP 20, PS 6 above PEEP 6
Past Medical History
• Medications
• Flovent 44 mcg 2 puffs bid
• Albuterol 4 puffs q4h prn cough/wheeze
• TobraDex topical prn stoma irritation
• Ibuprofen prn fever
•
•
•
•
All: Sulfa, latex
FH: Negative
SH: Lives with parents, developing well
EH: Negative
Physical Examination
• VS: 36.7 155 30 117/66 98% on 1.5L
• Gen: Well appearing.
• EENT: Mild conjunctival injection. TMs normal. Clear
rhinorrhea. OP clear.
• Neck: No cervical adenopathy
• Resp: RR 28-30 with 1+ inspiratory work. Symmetric
chest excursion. Diffusely coarse inspiratory BS without
wheezes or crackles. No prolongation of expiration.
• CV: Sinus tachycardia. Good pulses.
Physical Examination
• Stoma:
• 1-2 mm margin of erythema
• 3 mm granulation at 7:30 position
• 4 mm area of denudation at 3:30 position
• Mild-moderate thick greenish drainage
• No fluctuance, hematoma
Admission Labs
•
•
•
•
•
CBG 7.46/36; serum HCO3 26
WBC 26.1
CRP 6.2
Viral FA negative
Tracheal aspirate
• Gram stain: Few PMNs
• Culture: Pa, MSSA
7/16/07 (10 m/o)
7/19/10
12/17/10
1/31/11
CRP (mg/dL)
WBC (k/mm3) or Tmax (°C)
Clinical and Laboratory Trends
metronidazole 2/9-2/24
ceftaz+gent
pip/tazo
linezolid+cipro
Friday 4:00 PM Call
• Abundant growth of AFB within 48 hours on a fungal
plate
→ Mycobacterium abscessus
Never Saw That One Coming…
•
M. abscessus an unusual disease-causing pathogen
in this population
•
•
•
Uncommon cause of tracheitis
Tracheostomy nor BPD not considered a siginficant risk factor
Colonization versus infection?
•
•
•
Circumstances surrounding recovery of this pathogen
Clinical symptoms
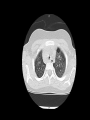
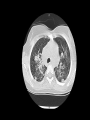
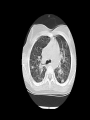
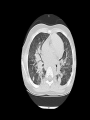
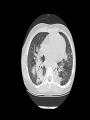
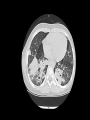
Radiographic disease
2007 ATS/IDSA Diagnostic Criteria
Microbiological Findings
• 3/2/11: Tracheostomy stoma site and a tracheal aspirate
both positive
• 3/9/11: BAL fluid positive
Rapidly Growing Mycobacteria (RGM)
• Subgroup of nontuberculous mycobacteria (NTM)
• Visible growth on solid media within 7 days
• Ubiquitous environmental organism
• Southern coastal states
• Water, soil, biofilm
M. abscessus Epidemiology
• RGM-specific incidence not definitively known
• Isolation: 1.51/100,000
• Disease: 0.39/100,000
• Most common clinical disorders due to RGM
• Skin/soft tissue infections
• Chronic lung disease (bronchiectasis, nodules, cavitations)
• M. abscessus
• Most common respiratory pathogen among RGM
• Third most common respiratory pathogen among all NTM
Risk Factors For M. abscessus Pulmonary Disease
•
•
•
•
•
Caucasian women, >60 years old, thin, nonsmoker
Prior TB infection/treatment
Gastroesophageal motility disorders
Cystic fibrosis
Alpha 1 antitrypsin deficiency
M. abscessus Treatment
• In vitro resistance to multiple
antibiotics
• Typical regimen
•
•
•
IV amikacin +
IV imipenem or cefoxitin +
PO clarithromycin
• Newer agents
•
•
•
Linezolid
Tigecycline
Telithromycin
Our Patient
• Admitted 3/21/11 to initiate antimicrobial therapy
• Inhaled amikacin
• IV tigecycline
• GT clarithromycin
Summary and Considerations
• Fevers of unknown origin in a 4 year old trach/vent child
• Stoma drainage, supplemental oxygen need, radiographic
findings
• “Reassuring” serial clinical examinations of the stoma
• Serendipitous isolation of M. abscessus
• Now that we’ve started therapy…
• Monitoring?
• Duration?
• Immune work-up?
Take Home Points For My Fellow Fellows
1. M. abscessus is a member of rapidly growing (≤7 days)
mycobacteria
2. Neither tracheostomy nor BPD are well-documented
risk factors for M. abscessus
3. 2007 ATS/IDSA guidelines
• Clinical symptoms
• Radiographic findings
• Confirmatory cultures
• ≥2 sputum from different samples or
• ≥1 bronchial or
• lung biopsy (granuloma/AFB + a positive culture)
Thank You!
References
1. Griffith DE et al. Am J Respir Crit Care Med. 2007;175:367-416.
2. Colombo RE et al. Semin Respir Crit Care Med. 2008;29:577-88.
3. Daley CL et al. Clin Chest Med. 2002;23:623-32.
4. Griffith DE. Curr Opin Infect Dis. 2010;23:185-90.
5. Nash KA et al. Antimicrob Agents Chemother. 2009;53:1367-76.
6. Esteban J et al. Eur J Clin Microbiol Infect Dis. 2008;27:951-7.
Cryptic Resistance
•
•
•
•
•
Macrolide antimicrobial agents act by binding to the 50S ribosomal subunit and
inhibiting peptide synthesis.
Erythromycin methylase (erm) genes code for methylases that impair binding of
macrolides to ribosomes
Inducible erm41 is the primary mechanism of acquired clinically significant macrolide
resistance for some mycobacteria, especially RGM
All isolates of M. abscessus, M. fortuitum and several other RGM, but not M.
chelonae, contain an inducible erm gene
If an M. fortuitum or M. abscessus isolate is exposed to macrolide, the erm gene
activity is induced with subsequent in-vivo macrolide resistance which may not be
accompanied by a change in the in-vitro MIC
Nash KA et al. Antimicrob Agents Chemother. 2009;53:1367-76.
Literature Search
•
("Tracheitis"[Mesh] OR "Tracheostomy"[Mesh]) AND "Mycobacteria, Atypical"[Mesh]
•
•
•
•
“Administration,Inhalation”[Mesh] AND "Mycobacteria, Atypical"[Mesh]
•
•
Kasai S et al. [A case of bronchial ulcer due to infection by Mycobacterium abscessus].
Nihon Kokyuki Gakkai Zasshi. 2004;42:919-23. Japanese.
Levashev IuN et al. [Circular resection of the upper trachea for concomitant postintubation
cicatricial stenosis and mycobacterial lesion]. Probl Tuberk Bolezn Legk. 2003;10:61-3.
Russian.
Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises.
Case 33-1996. A 55-year-old man with a long-term tracheostomy and acid-fast bacilli in
peristomal granulations. N Engl J Med. 1996;335:1303-7.
Wang BY et al. Atypical mycobacteriosis of the larynx: an unusual clinical presentation
secondary to steroids inhalation. Ann Diagn Pathol. 2008;12(6):426-9.
"Bronchopulmonary Dysplasia"[Mesh] AND "Mycobacteria, Atypical"[Mesh]
•
No items found