Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
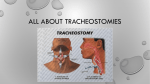
2. You work in a rural emergency department with only basic specialties represented. An 80 year old man is delivered to your emergency department with an acute anterior ST elevation myocardial infarction. He developed severe central chest pain two hours ago which is ongoing. He is anxious, pale and diaphoretic. Widespread crepitations can be heard throughout his lung fields. Your local retrieval helicopter is out on another job and you have no alternative retrieval options available for at least 4 hours. His observations are: GCS 15 HR 100 beats/min (regular) BP 190/105 mmHg RR 24 /min O2 Saturation 91 % on air Temperature 36.8 oC a) Outline 5 key treatment priorities for this man. 1. 2. 3. 4. 5. 6. Basic initial stabilisation (bilateral large bore IV access, application of O2, apply defib pads) Early adjunctive therapy for STEMI (aspirin, morphine for pain) Acute reperfusion with thrombolysis Chemical management of APO with GTN infusion NIV to improve gas exchange Supportive cares – high mortality so identifying goals of care, involvement of family b) List four indications for NIV Parameters Respiratory rate (breaths/min) Normal range 10 - 20 Ventilatory support > 30 for Type I > 24 for Type II Features of respiratory fatigue Absent Abdominal paradox Tidal volume (mL/kg) 5-7 <5 Vital capacity(mL/kg) 65 - 75 < 15 PEFR (L/min/kg) 7-10 < 1.5 Maximum inspiratory force (cm H2O) 75 - 100 < 25 paO2 mmHg 75 - 100 on air < 60 on 50% O2 (or PaO2/FiO2 > 200) pCO2 mmHg 35 - 45 > 60 Response to therapy Adequate Poor (Dunn pg 50) c) What primary complications would you anticipate in initiating NIV for this man? Hypotension (poor LV fn, concomitant nitrates, reduced venous return from IPPV) Poor compliance (due to distress, ALOC, discomfort) Excessive respiratory secretions d) How would you treat this complication should it arise? cease vasodilators maximise oxygenation small fluid challenge with colloid if oxygenation satisfactory inotropic agents if oxygenation poor and unable to be improved (Dunn pg 57) 3. A baby is born in your resuscitation room after a precipitous birth from a 32 week pregnant woman. The baby is not breathing and there is thick meconium stained liquor on the bed. The delivery is otherwise uneventful and the mother requires no acute medical treatment. There is no on-site neonatal or obstetric service. a) List 8 key steps in resuscitation of the preterm newborn. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. keep infant warm (resuscitaire) clear meconium from airway with suction dry and stimulate infant to breathe post clearing meconium provide PPV if infant not breathing and/or HR<100bpm Endotracheal intubation considered early due to prematurity and meconium aspiration Circulation – provide ECC + PPV @ 3:1 if HR<60bpm Adrenaline if HR<60bpm Establish access (IV periph/umbi, or IO) Estimated weight 2-3kg Assigned person to support mother b) List your differential diagnosis. • N iNborn errors of metabolism • E electrolyte abnormalities • O overdose (toxin, poison) • S seizures • E enteric emergencies • C cardiac abnormalities • R recipe (formula, herbs, additives) • E endocrine crisis • T trauma • S sepsis (Dunn pg 145) c) Outline your post-resuscitation care in this situation - - Early consultation with neonatal retrieval services Consideration of all causes in DDx, including initiation of any appropriate medications: o Glucose o Antibiotics o Anti-epileptics o Naloxone Observation and monitoring while awaiting transfer Care of mother Psychosocial care of parents and family Transfer to tertiary centre with NICU/SCN 8. A 65 year old man is brought to hospital by ambulance from home. He was found in an agitated state with extreme respiratory distress, breathing through a tracheostomy tube. He was hot to touch and combative. During unloading from the ambulance trolley in the emergency department he loses consciousness and stops breathing. He is taken immediately to the resuscitation room. a) What is your immediate treatment priority? Commencement of CPR, or confirm perfusing rhythm follow ALS protocol b) List your differential diagnosis. Upper airways obstruction Sepsis PE MI Hypoxia Hypovolaemia Tamponade Hyperkalaemia Toxins Tension PTX c) List 4 key features to consider when managing a tracheostomy. Check whether tracheostomy is cuffed/uncuffed Suction the tracheostomy tube. Change the patient’s inner cannula tube/sheath if one is present. Extend the patient’s neck slightly with a small towel rolled under the shoulders. If the tracheostomy tube is still blocked or dislodged: remove and re-insert a new tube. If unable to re-cannulate, try again using a smaller size tube. IF NOT BREATHING – connect tracheostomy tube to Bag-Valve and ventilate, ensuring no air leaks through nose/mouth IF BREATHING – connect tracheostomy mask with high-flow oxygen d) List 4 principles which would favour withdrawal of resuscitation. Unnecessary – easily fixed by measures outlined above Unsuccessful / Futile – prolonged arrest, Unkind – expected outcome likely to bring about an outcome devastating to patient and/or family Unwise – disproportionate diversion of resources which may be required elsewhere Unwanted – DNR/AHD/substitute decision maker (Cameron 15-17)