Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
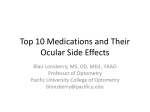
Grand Rounds Mark Mugavin M.D., MPH University of Louisville School of Medicine Department of Ophthalmology & Visual Sciences 8/21/2015 Subjective CC: blurry vision OU HPI: 57 year old white female with a history of B Cell Acute Lymphoblastic Leukemia (ALL) s/p bone marrow transplant March 2015 currently admitted on BMT service with abdominal pain, diarrhea, malaise, palpable pruritic skin patches. Subjective Patient has noticed episodes of blurry vision more frequent in the morning and noticeable at distance Episodes lasting approximately 2-3 hours a day since being admitted a week ago. POH: presbyopia PMHx: ALL s/p transplant, Adult Polycystic Kidney Disease ROS: per hpi. No visual disturbance noted in months leading up to admission Medications: Tacrolimus, Solumedrol 2 mg per kg IV Allergies: NKDA Social: social alcohol, denies cigarettes or illicits Exam OD OS VA(cc, near): 20/20-2 +2.00 20/25 +2.00 Pupils: 4 4 2 2 No APD IOP: EOM 15 17 0 0 0 0 0 0 0 0 Exam OD OS Anterior Segment L/L Madarosis C/S: Clear Cornea: AC: I/L: Vitreous: DFE: Few scattered SPK Dry eye Madorosis Mild Palpebral Conjunctival Hyperemia Diffuse SPK, Severe Dry Eye No cell or flare OU WNL OU WNL OU WNL OU Clinical Photos Clinical Video Additional Considerations While on high dose solumedrol last 6 Glucose readings (139,186,169,248,263,229) Differential Diagnosis Graft vs Host Disease with Ocular Manifestations Hyperglycemic Induced Refractive Error Assessment and Plan 59 year white female s/p BMT for ALL currently inpatient for Graft Host Disease. positive rose bengal staining, minimal conjunctival hyperemia OS Prescribed artificial tears (preservative free) every 2 hours while awake for active lubrication. Lacrilube at hours of sleep Hematopoetic Stem Cell Transplants Epidemiology Est. 20,000 performed annually in U.S. Top three indications: Multiple Myeloma, NonHodgkins Lymphoma, Acute Myelogenous Leukemia 1958 French Oncologist Georges Mathe Performed first BMT following nuclear accident in Yugoslavia 1950’s-1960’s Dr. Donnal Thomas often cited as pioneer of the field found matching related dogs critical to success. Leader of Fred Hutchinson Cancer Research Center (Seattle). Nobel Prize in 1990 Graft vs Host Dx (GVD) Acute Classically defined as developing in first 100 days Involves mucous membranes of mouth, intestinal tract, skin, liver HLA Identical Siblings 19-66% vs Matched Unrelated 70-90% Chronic >100 days and onwards Involves lungs, eyes, and intestines HLA Identical Siblings 33% vs Matched Unrelated 64% Most studies suggest incidence of 60-90% overall GVHD Pathophysiology Complex multistep process with 3 essential criteria: a) Graft must contain immunologically competent cells b) Host must possess transplantation antigens lacking in the graft which appear foreign, thereby stimulating donor T cells c) Host must be incapable of mounting a reaction against the graft for a period of time sufficient to allow the graft cells to attack the host Ocular GVHD Donor T cells (CD 4/ CD 8) are stimulated through cytokines (IL1, IL2, interferon gamma, TNF-A) to attack the lacrimal glands, conjunctiva, and accessory tear glands Aqueous deficiency can lead to diminished visual acuity, corneal ulceration, microbial keratitis Formation of a conjunctival pseudomembrane associated with poor prognosis CD45+ Positive Staining of inflammatory T cells attacking lacrimal duct of a 21 yo male with Chronic GVHD (Photo credit #3 Ogawa et al) Ocular GVD Clinical Symptoms keratoconjunctivits sicca (#1) confluent areas of punctate keratopathy new onset dry, gritty painful eyes cicatricial conjunctivitis Assessing Ocular GVHD Slit Lamp Examination Dye Staining of Conjunctiva, Cornea (Fluorescein, Rose Bengal, Lissamine green) Assessment of tear film utilizing Schirmer test, chemical analysis, microscopy Schirmer Test - 5 mm or less diagnostic - 6-10 mm with another organ impacted suggestive Grading GVHD Grade 1: Conjunctival hyperemia occurring on the bulbar or palpebral conjunctiva in at least one eyelid Grade 2: Palpebral conjunctival fibrovascular changes occurring along the superior border of the upper eyelid or lower border of the tarsal plate < 25% Grading GVHD Grade 3: palpebral conjunctival fibrovascular changes involving 25 to 75% of at least one eyelid Grade 4: > 75% involvement with or without cicatricial entropion Management Most resources recommend a stepwise approach 1)Preservative Free Artificial Tears and Viscous Ointment at bedtime 2) Autologous Tears 3) Mucolytic agents (ex: 10% N-Acetylcysteine) 4) Punctual Plugs 5) Topical Corticosteroids 6) Cyclosporine A 7) Tacrolimus 8) Scleral Large Diameter Contact Lenses Literature Review Scleral Contact Lenses Large diameter, rigid, gas permeable lenses designed to cover exposed ocular surface Features a) b) c) Rest on the conjunctival tissue overlying the sclera in a way that vaults the cornea and limbus Contain post-lens fluid reservoir for continuous hydration Protection of the cornea and conjunctivae from irritation caused by lid movement over the ocular surface Scleral Lenses Scleral Contact Lens Patient with prominent Ocular GVD fitted with Scleral Contact Lens. Note the sub-epithelial scarring on the inferior paracentral cornea Slit lamp view demonstrating the space present between the cornea and the contact lens Evidence for Scleral Lenses Retrospective study from Harvard(n=33) patients with Chronic GVHD that failed “conventional therapy” (Enrollment Dec 2002 to Feb 2005) Fitted with Boston Scleral Lenses and basic assessment of satisfaction measured 97% reported less eye pain 94% reduction in photophobia 93% improvement in reading Scleral Lenses References 1. Balasubramian et al. “Ocular Graft-Versus-Host-Disease: A Review” Eye and Contact Lens 2015; 0 1-7 2. Lin X, Cavanagh H “Ocular manifestations of graft-versus-host disease: 10 years experience” Clinical Ophthalmology 2015 July 3; 9 1209-1213 3. Ogawa et al. “International Chronic Ocular Graft-vs-Host Disease (GVHD) Consensus Group: Proposed Diagnostic Criteria for Chronic GVHD” Nature. Scientific Reports 3: Article 3419 (2013) 4. Pezzotta S, Rossi G, “A cross sectional study on vision-related quality of life in patients with Ocular GvHD Bone Marrow Transplantation 8 June 2015 5. “Transplant Activity Report 2008-2012” Health Resources and Service Administration Blood Cell Transplant http://bloodcell.transplant.hrsa.gov/research/transplant_data/transplant_activity_report/index.html#numbers 6. “Ocular Graft Versus Host Diease” BCSC Section 9: External Disease and Cornea American Academy of Ophthalmology 2015 Additional Info