Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
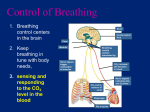
The Respiratory System The Respiratory System Functions: – To provide the body with means of taking in(O2) for the production of ATP and eliminating (CO2) a byproduct of aerobic respiration. – To help maintain the body’s pH, by regulating the blood CO2 levels in the body. – Work in conjunction with the cardiovascular system to move these gases from the lungs to the cells and from the cells to the lungs. Organs of Respiratory System Conducting Zone • Conducting zone – Provides rigid conduits for air to reach the sites of gas exchange – Respiratory structures include (nose, nasal cavity, pharynx, trachea, primary, secondary and tertiary bronchi) – No Gas exchange Respiratory Zone • Respiratory zone: – begins as terminal bronchioles → respiratory bronchioles → alveolar ducts, → alveolar sacs composed of alveoli – This is where gas exchange occurs! Nose • Functions – Nasal choanae creates turbulent air flow that allows air to contact mucus membranes and superficial nasal sinuses. • The result is cleaner, warmer more humidified inhaled air. – detects odors via the olfactory cranial nerve which also enhances our sense of taste. – Resonating chamber that amplifies the voice Pharynx Larynx • Larynx (“voice box”) – contains vocal cords allowing speech production • Glottis – vocal cords • Epiglottis – flap of tissue that guards glottis, directs food and drink to esophagus Trachea • Flexible and mobile tube extending from the larynx to the carina (split into primary bronchi) • Composed of three layers – Mucosa – made up of pseudostratified ciliated epithelium that contain goblet cells that secrete mucus to trap dirt. • Mucociliary escalator: cilia beats in an upward fashion toward the pharynx where debris can be swallowed. – Submucosa – connective tissue deep to the mucosa – Adventitia – outermost layer made of C-shaped rings of hyaline cartilage which prevent the airway from collapsing. Trachea Respiratory Zone • Approximately 300 million alveoli: – Account for most of the lungs’ volume – Provide tremendous surface area for gas exchange – Equivalent to 2 tennis courts in surface area. Respiratory Membrane Respiratory Membrane Air-blood barrier is composed of alveolar and capillary walls. – Alveolar walls: contain 2 main types of cells 1. Type I epithelial cells (simple squamous epithelium) that permit gas exchange by simple diffusion 2. Type II cells (cuboidal epithelium ) secrete surfactant which enables the lungs to expand. 3. White blood cells are found in the lumen of the alveoli. 1. Function to protect against infections from inhaled pathogens 4 Processes of Respiration 1. Pulmonary ventilation – air moving into and out of the lungs along their pressure gradients. • • Inspiration – air(O2)flows into the lungs Expiration – air (CO2) exit the lungs 2. External respiration – gas exchange between the lungs (alveolus) and the blood (pulmonary capillaries) 3. Transport – transport of oxygen and carbon dioxide between the lungs and tissues via the circulatory system. 4. Internal respiration – gas exchange between systemic blood vessels (capillaries) and the tissues (cells) • Gases must diffuse into interstitial fluid prior to any exchange between the tissue and the cell. Pulmonary Ventilation • Taking of air into and out of the lungs. • A mechanical process that depends on respiratory muscles changing the size of the thoracic cavity – Because this cavity is connected to the lungs via the parietal membranes it may also influence the lung (alveolar )volume. • A increase in alveolar volume will move air into the lungs down it concentration gradient. • A decrease in alveolus volume will move air out of the lungs. Boyle’s Law • The changes in thoracic volume is necessary to move air in and out of the lungs. The movement of air in dependant of: – Boyle’s law – Pressure and Volume are inversely proportional. • P ×V= Constant • If pressure increases volume decreases • If pressure decreases volume increases and vise versa • This mechanism is dependent on a doublelayered membrane system called (Pleurae) Pleurae Parietal pleurae Visceral pleurae Intrapleural space Pleurae • Parietal pleura – Covers the thoracic wall and superior face of the diaphragm – Continues around heart and between lungs Visceral pleura – Covers the external lung surface • Intrapleural Space – Space between the parietal and visceral pleurae. – There is a small amount of fluid (pleural fluid) within the space that hold the 2 pleurae together • This will reduce friction between the lungs and the thoracic cavity. – Similar to a small amount of water between 2 plains of glass. • Slides easily but difficult to separate. Pulmonary Pressures • Intrapulmonary pressure and intrapleural pressure fluctuate with the phases of respiration. – Intrapulmonary pressure aka. alveolar is the pressure with in the alveolus – Intrapleural pressure is the pressure within the pleural space • created by many hydrogen bonds between the water molecules of the pleural fluid. • Intrapleural pressure must always less than intrapulmonary pressure and atmospheric pressure Pulmonary Pressures Intrapulmonary pressure Atmospheric pressure intrapleural pressure Lung Collapse • Caused by equalization of the intrapleural pressure with the intrapulmonary pressure • Transpulmonary pressure keeps the airways open – Transpulmonary pressure – difference between the intrapulmonary and intrapleural pressures (Ppul – Pip) Muscles of Respiration Inspiration Expiration Figure 22.13.2 Respiratory muscles • The muscles collectively work to change the volume of the thorax during ventilation. • Inspiration – Diaphragm via the phrenic nerve flattens out increasing thoracic volume depth – External intercostals via intercostal nerves pull the ribs up and out. • This collectively increase the size (volume) of the thorax and the lungs via its attachment to the pleura. • Expiration – Normal expiration is a passive process that involves the relaxation of the inspiratory muscles. – Forced expiration is an active process involving the internal intercostals and abdominals contracting forcing the ribs down decreasing the size (volume) of the thorax. • coughing • What is the mechanism of action for the Heimlich Maneuver? Lung Compliance • The lungs ability to expand despite the lungs tendency to collapse. • Determined by two main factors: – Distensibility of the lung tissue and surrounding thoracic cage – Reducing surface tension of the alveoli: as the lungs expand it stretches the type II cell to produce more surfactant. • Surfactant is a detergent-like complex, reduces surface tension by breaking H-bonds allowing the lungs to expand. Factors That Diminish Lung Compliance • Scar tissue or fibrosis that reduces the natural resilience of the lungs preventing them to expand during inhalation. • Blockage of the smaller respiratory passages with mucus or fluid • Reduced production of surfactant • Decreased flexibility of the thoracic cage or its decreased ability to expand • Examples include: – Deformities of thorax – Ossification of the costal cartilage – Paralysis of intercostal muscles Deformities of Thorax • Barrel Chest Pectus Excavatum Environmental Influences of Ventilation: • The amount of gas flowing into and out of the alveoli is directly proportional to Pressure – The greater the pressure gradient between the atmosphere and the alveoli the more air will enter the lungs • Atmospheric pressure (Patm) – Pressure exerted by the air surrounding the body • Altitude and (Patm) are inversely proportional. – It is much easier to breath at sea level than it is a 10,000 ft above. Why? Airway Resistance • Gas flow is inversely proportional to resistance – The resistance increases as vessel diameter decreases. • This will lead to less gas reaching the alveoli for exchange. • As airway resistance rises, breathing movements become more strenuous – Severely constricted or obstructed bronchioles: • Can occur during acute asthma attacks which stops ventilation . – Epinephrine released via the sympathetic nervous system or medically induced dilates bronchioles and reduces air resistance. Dalton’s Law of Partial Pressures • The air that we breath is made up of 4 main gases – N2, O2, H2O and CO2 – There is a different % of each of the above gases in the atmospheric air. – Each gas therefore makes up a different proportion of the total mixture. • The sum of the partial pressures of each individual gas is equal to the total pressure of the air. • The partial pressure of the various gases are important in establishing the gradients which drives the gases throughout the system. Partial Pressure Gradients Partial Pressures Gradients During Internal Respiration • PCO2 (45mmHg) in peripheral tissues is higher than in the arteries returning from the lungs(40mmHG) because CO2 is a end product of cellular respiration. • The PO2(40mmHg)is lower in the tissues than the arterial blood (95mmHg) because O2 is being continuously being used by the cells. • O2 and CO2 will diffuse along their concentration gradients – O2 from blood to tissues – CO2 from tissue to blood Partial Pressure Gradients During External Respiration • Following (internal respiration)O2 unloading to the tissues and CO2 uptake into the blood the (PO2) in venous blood decreases to 40 mmHg and the PCO2 increases to 45mmHg • Following ventilation the PO2 in the alveoli is104 mmHg and PCO2 decreases to 40mmHg • O2 and CO2 will diffuse along its pressure gradient from high to low – – – – PO2 =lungs → blood CO2 = blood → lungs Diffusion will occur until equilibrium is met. Blood PO2 and PCO2 will = the alveolus partial pressures. Gas Transport: Role of Hemoglobin • Molecular oxygen is carried in the blood: – Bound to hemoglobin (Hb) within red blood cells (99%) • The hemoglobin-oxygen combination is called oxyhemoglobin (HbO2) – Dissolved in plasma (1%) • Carbon dioxide is transported in the blood in three forms – Dissolved in plasma – 7 to 10% – Chemically bound to hemoglobin – 20% is carried in RBCs as carbaminohemoglobin – Bicarbonate ion in plasma – 70% is transported as bicarbonate (HCO3–) Internal Respiration Internal Respiration CO2 Carbon dioxide + H2O Water H2CO3 Carbonic acid H+ Hydrogen ion + HCO3– Bicarbonate ion At the tissues: • Carbon dioxide diffuses into RBCs • The high concentration of CO2 causes the above equation to shift to the right. – combines with water to form carbonic acid (H2CO3) • (H2CO3), which quickly dissociates into hydrogen ions and bicarbonate ions • Hydrogen ions attach to one of 4 heme molecules in the RBC dislodging on of the O2 (Bohr effect) – Oxygen travels down its concentration gradient to the tissues • Bicarbonate levels quickly build up and will quickly diffuses from RBCs into the blood plasma • The chloride shift – to counterbalance the out rush of negative bicarbonate ions from the RBCs, chloride ions (Cl–) move from the plasma into the erythrocytes External Respiration External Respiration CO2 Carbon dioxide + H2O Water H2CO3 Carbonic acid H+ Hydrogen ion + HCO3– Bicarbonate ion • When the blood gets to the lungs these processes are reversed. – The above reaction will shift to the left. • Bicarbonate ions move into the RBCs and bind with hydrogen ions to form carbonic acid • Carbonic acid is then split by carbonic anhydrase to release carbon dioxide and water – CO2 levels quickly rise in the cell • CO2 diffuses from the blood into the alveoli along its concentration gradient. Oxygen-Hemoglobin Dissociation Curve • The higher the PO2 in the blood the greater the percent O2 saturation. • The percent O2 saturation plotted against blood PO2 – this tells us the amount of oxygen that is bound to hemoglobin at a particular PO2 in the blood – We monitor O2 saturation levels with patients with pulmonary issues • Below 90% is termed hypoxemia Other Factors Influencing Hemoglobin Saturation • Increases in Temperature, H+, PCO2, and BPG increase O2 unloading from the hemoglobin. – This will result in a shift to the right on the curve • When the cells are more metabolically active there is a greater need for O2. • Temperature increases in metabolically activity, the tissues because heat is a byproduct of cellular respiration. • Active cells will also produce more CO2 and H20 which ultimately will lead to greater amounts of H+ – Both these byproducts ensure that O2 will be unloaded from the RBC and delivered to the tissues. • Decreases in Temperature, H+, PCO2, and BPG will act in the opposite manner – This will result in a shift to the left on the curve Factors Influencing Hemoglobin Saturation Medullary Respiratory Centers • Ventral Respiratory Group: Sets the underline breathing rate .It activates the – Diaphragm stimulated via the Phrenic Nerve – External Intercostals stimulated via the Costal Nerves • Dorsal Respiratory Group (DRG): receives input from multiple areas. – It modulates the breathing rate of the VRG so it can adapt to various situations. Pons (Secondary Centers) • Apneustic Center • Stimulation of this center causes strong inspirations or aids in prolong inspiration. • stimulations the inspiratory center • Pneumotaxic Center • inhibits the VRG to end inspiration – provides for a smooth transition between inspiration and expiration • Stimulation of this center inhibits the Apneustic center • Contributes to expiration • Cortical control: we can actively effect our respiratory rate such as • holding breath under water • The Limbic system and hypothalamus also stimulate the respiratory centers. • Emotional effect on respiration Depth and Rate of Breathing: Reflexes • Inflation reflex (Hering-Breuer) – stretch receptors in the lungs are stimulated by lung inflation – Upon inflation, inhibitory signals are sent to the medullary inspiration center to end inhalation and allow expiration • Pulmonary irritant reflexes – irritants promote reflexive constriction of air passages Central Chemoreceptors • Changing PCO2 levels are monitored by Central chemoreceptors of the brain stem – Carbon dioxide in the blood diffuses into the cerebrospinal fluid – CO2 + H2O H2CO3 HCO3- + H+ • PCO2 levels rise (hypercapnia) resulting in increase in H+ ion level concentration in the medulla. • This stimulations of( DRG) increased depth and rate of breathing – CO2 (expired) + H2O H2CO3 HCO3- + H+ • This will allow the body to blow off more CO2 thus reducing CO2 levels reestablishing homeostasis. Depth and Rate of Breathing: PCO2 Peripheral Chemoreceptors • Arch of the Aorta – main vessel originating from the heart • Carotid sinus – main artery in the neck • Elevated arterial P CO2 and H+ ion concentration or decrease in PO2 will stimulate DRG to increase respiratory rate. – CO2 levels are the main driving force behind respiratory rate. Depth and Rate of Breathing: PCO2 • Hypoventilation – When PCO2 levels are abnormally low the body will slow its respiratory rate. – Holding your breath or breathing slow and shallow will cause CO2 levels to start to raise in your blood • As the CO2 levels start to rise again this will trigger chemoreceptors to stimulate DRG to increase ventilation causing thus exhaling more CO2 levels in the blood CO2 – Apnea (breathing cessation) may occur until PCO2 levels rise Depth and Rate of Breathing: PCO2 • Hyperventilation – increased depth and rate of breathing that: – Quickly flushes CO2 from the blood • CO2 (expired) + H2O H2CO3 HCO3- + H+ – Occurs in response to hypercapnia( high CO2 in blood) • Though a rise CO2 acts as the original stimulus, control of breathing at rest is regulated by the hydrogen ion concentration in the brain • Why do you give someone a bag to breath into if they are hyperventilating? Respiratory Acidosis • pH of CSF (most powerful respiratory stimulus) • Respiratory acidosis (pH < 7.35) caused by decline in pulmonary ventilation ( not blowing CO2 off) • PCO2(Normal 35-45)=>45 Acidic – hypercapnia: PCO2 > 45 mmHg • CO2 easily crosses blood-brain barrier • in CSF the CO2 reacts with water and releases H+ – CO2 + H2O H2CO3 HCO3- + H+ • central chemoreceptors strongly stimulate inspiratory center (DRG) stimulates phrenic and intercostal nerve which targets inspiratory muscles increasing respiratory rate. – “blowing off ” CO2 pushes reaction to the left CO2 (expired) + H2O H2CO3 HCO3- + H+ • so hyperventilation reduces H+ (reduces acid) Respiratory Alkalosis • Respiratory alkalosis (pH > 7.35) – hypocapnia: PCO2 < 35 mmHg • CO2 (expired) + H2O H2CO3 HCO3- + H+ – Hypoventilation ( CO2), pushes reaction to the right CO2 + H2O H2CO3 HCO3- + H+ – H+ (increases acid), lowers pH to normal • pH imbalances can have metabolic causes – uncontrolled diabetes mellitus • fat oxidation causes ketoacidosis, may be compensated for by Kussmaul respiration (deep rapid breathing) Hypoxia • Causes: Reduced levels of oxygen particularly in the blood. – hypoxemic hypoxia - usually due to inadequate pulmonary gas exchange • high altitudes, drowning, aspiration, respiratory arrest, degenerative lung diseases, CO poisoning – ischemic hypoxia - inadequate circulation • DM, Atherosclerosis – anemic hypoxia – anemia • Diet and internal bleed – histotoxic hypoxia - metabolic poison • cyanide poisoning • Signs: cyanosis - blueness of skin, finger nail clubbing • All types of hypoxia can lead to tissue necrosis ( death) Signs of Cyanosis Chronic Obstructive Pulmonary Disease • Asthma – Chemical irritants cause the release of release of histamine which activates the PNS. This leads to intense bronchoconstriction (blocks air flow) – Treatment is Epinephrine. Why? • Other COPD’s usually associated with smoking – chronic bronchitis – emphysema Chronic Bronchitis • Chronic Bronchitis typically occurs in the larger airways. • Patients have a history of: – Smoking – Dyspnea: labored breathing occurs and gets progressively worse – Coughing and sputum production leading to frequent pulmonary infections. • COPD patients may develop respiratory failure accompanied by hypoxemia, carbon dioxide retention resulting in respiratory acidosis Chronic Obstructive Pulmonary Disease • Emphysema – An inflammatory response destroys the alveolar walls ( respiratory membrane) reducing the surface area for gas exchange – Lungs become more fibrotic and less elastic – Air passages collapse with exhalation trapping CO2 in lungs. Effects of COPD • pulmonary compliance and vital capacity • Hypoxemia, hypercapnia, respiratory acidosis – hypoxemia stimulates erythropoietin release and leads to polycythemia • cor pulmonale – hypertrophy and potential failure of right heart due to obstruction of pulmonary circulation Smoking and Lung Cancer • Lung cancer accounts for more deaths than any other form of cancer – most important cause is smoking (15 carcinogens) – If you smoke the equivalent of 50 pack years your chance of getting lung cancer is 100% • 50% of smokers die from smoke related illness.